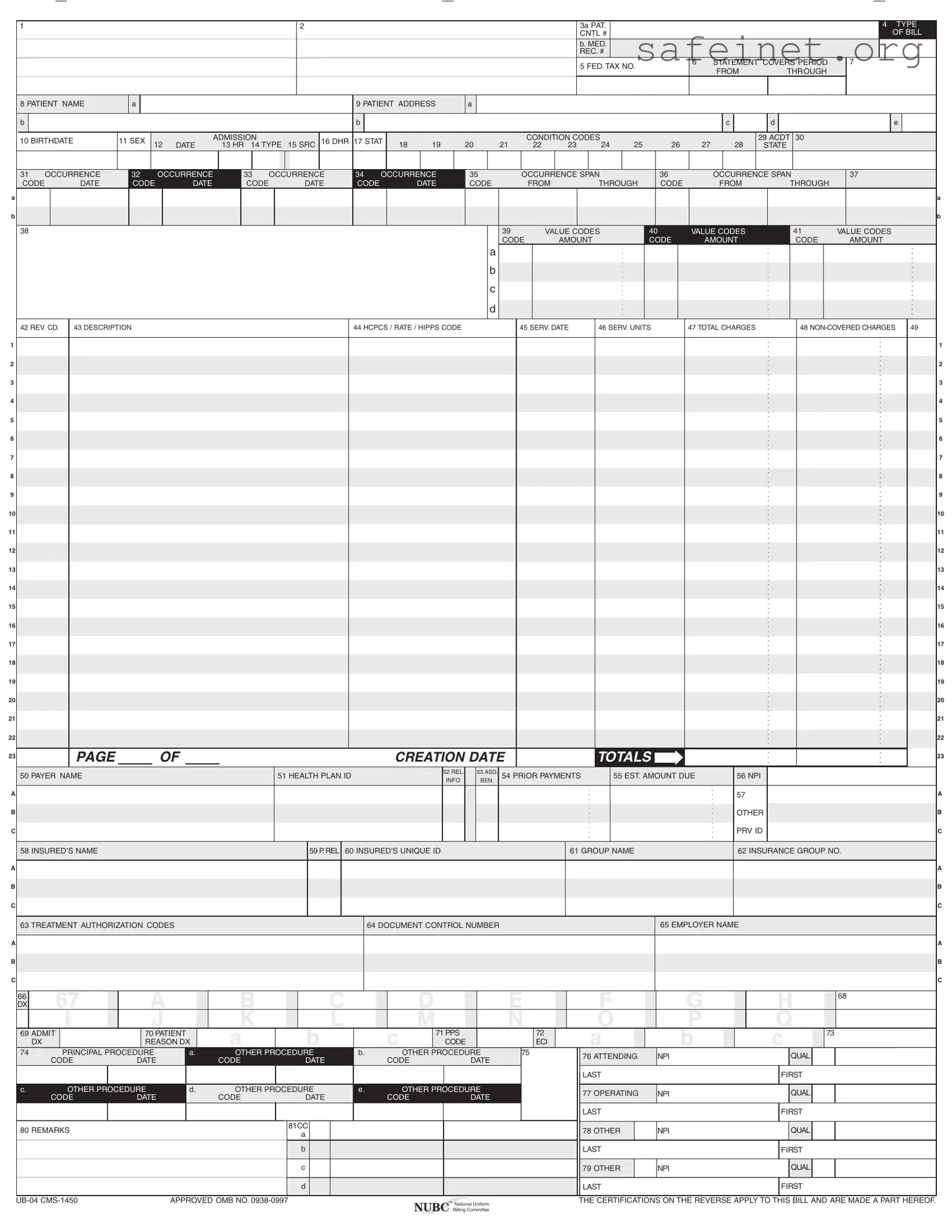
The UB-04 form, also known as the CMS-1450, plays a crucial role in the healthcare billing process, serving as a standardized claim form for institutional providers. This form captures a comprehensive array of information about patient care, including demographic details, service dates, and specific charges associated with medical treatments. Each section of the UB-04 is meticulously designed to ensure accurate reporting of services rendered, from patient identification to the detailed description of procedures performed. Notably, it includes codes for diagnosis, revenue, and procedures, which are essential for proper reimbursement from insurance providers. Additionally, the form requires certifications and verifications, affirming the authenticity of the information submitted. These certifications safeguard against potential legal ramifications, emphasizing the importance of accuracy and transparency in billing practices. The UB-04 is not just a form; it is a vital document that facilitates communication between healthcare providers and insurers, ensuring that patients receive the coverage they need while providers are compensated fairly for their services.
A
B
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
A
B
C
A
B
C
A
B
C
1 |
2 |
3a PAT. |
|
|
|
|
|
4 TYPE |
|
|
CNTL # |
|
|
|
|
|
OF BILL |
|
|
b. MED. |
|
|
|
|
|
|
|
|
REC. # |
|
|
|
|
|
|
|
|
5 FED. TAX NO. |
6 |
STATEMENT COVERS PERIOD |
7 |
|
||
|
|
|
FROM |
THROUGH |
|
|
||
|
|
|
|
|
|
|
||
8 PATIENT NAME |
a |
|
|
|
|
9 PATIENT ADDRESS |
a |
|
|
|
|
|
|
|
|
|
|
||
b |
|
|
|
|
|
b |
|
|
|
|
|
|
|
|
|
|
c |
d |
e |
10 BIRTHDATE |
11 SEX |
|
|
ADMISSION |
|
16 DHR 17 STAT |
|
|
|
|
CONDITION CODES |
|
|
|
|
|
29 ACDT 30 |
|
|
12 |
DATE |
13 HR 14 TYPE |
15 SRC |
18 |
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
STATE |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31 OCCURRENCE |
32 |
|
OCCURRENCE |
33 |
OCCURRENCE |
34 |
OCCURRENCE |
35 |
|
|
|
OCCURRENCE SPAN |
|
36 |
|
|
|
OCCURRENCE SPAN |
|
37 |
|
|
|
||||||||||||||||||||||||||||||
CODE |
DATE |
CODE |
|
DATE |
CODE |
|
|
|
DATE |
CODE |
|
DATE |
CODE |
|
|
|
FROM |
THROUGH |
|
CODE |
|
|
FROM |
|
THROUGH |
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
38 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
39 |
|
|
VALUE CODES |
40 |
|
|
VALUE CODES |
|
41 |
|
VALUE CODES |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CODE |
|
AMOUNT |
|
|
|
CODE |
|
|
AMOUNT |
|
CODE |
|
AMOUNT |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
42 REV. CD. |
43 DESCRIPTION |
|
|
|
|
|
|
|
|
|
|
|
|
|
44 HCPCS / RATE / HIPPS CODE |
|
|
|
|
45 SERV. DATE |
46 SERV. UNITS |
47 TOTAL CHARGES |
|
|
48 |
49 |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAGE |
|
|
OF |
|
|
|
|
|
|
|
|
|
|
CREATION DATE |
|
|
|
|
|
|
|
TOTALS |
|
|
|
|
|
|
|
|
|
|
|
|
|
23 |
|||||||||||||||
50 PAYER NAME |
|
|
|
|
|
|
|
|
51 HEALTH PLAN ID |
|
|
|
|
52 REL. |
|
53 ASG. |
54 PRIOR PAYMENTS |
|
55 EST. AMOUNT DUE |
|
|
56 NPI |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFO |
|
BEN. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
57 |
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRV ID |
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
58 INSURED’S NAME |
|
|
|
|
|
|
|
|
|
|
|
59 P. REL |
60 INSURED’S UNIQUE ID |
|
|
|
|
|
|
|
|
61 GROUP NAME |
|
|
|
|
|
|
|
62 INSURANCE GROUP NO. |
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
63 TREATMENT AUTHORIZATION CODES |
|
|
|
|
|
|
|
|
64 DOCUMENT CONTROL NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
65 EMPLOYER NAME |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C
66 |
67 |
A |
|
B |
|
C |
|
D |
|
E |
F |
G |
H |
68 |
DX |
|
|
|
|
|
|||||||||
|
I |
J |
|
K |
|
L |
|
M |
|
N |
O |
P |
Q |
|
69 ADMIT |
70 PATIENT |
|
A |
B |
|
C |
71 PPS |
|
72 |
A |
B |
C |
73 |
|
|
DX |
REASON DX |
|
CODE |
|
ECI |
|
|||||||
74 |
PRINCIPAL PROCEDURE |
a. |
OTHER PROCEDURE |
b. |
|
OTHER PROCEDURE |
75 |
76 ATTENDING |
NPI |
QUAL |
|
|||
|
CODE |
DATE |
|
CODE |
DATE |
|
CODE |
DATE |
|
|
||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
LAST |
|
FIRST |
|
c. |
OTHER PROCEDURE |
d. |
OTHER PROCEDURE |
e. |
|
OTHER PROCEDURE |
|
77 OPERATING |
NPI |
QUAL |
|
|||
|
CODE |
DATE |
|
CODE |
DATE |
|
CODE |
DATE |
|
|
||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
LAST |
|
FIRST |
|
80 REMARKS |
|
|
|
81CC |
|
|
|
|
|
78 OTHER |
NPI |
QUAL |
|
|
|
|
|
a |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b |
|
|
|
|
|
LAST |
|
FIRST |
|
|
|
|
|
|
c |
|
|
|
|
|
79 OTHER |
NPI |
QUAL |
|
|
|
|
|
|
d |
|
|
|
|
|
LAST |
|
FIRST |
|
APPROVED OMB NO. |
™ National Uniform |
THE CERTIFICATIONS ON THE REVERSE APPLY TO THIS BILL AND ARE MADE A PART HEREOF. |
|
|
|
NUBC Billing Committee |
|
| Fact Name | Description |
|---|---|
| Form Purpose | The UB-04 form is used for billing institutional healthcare providers for services rendered to patients. |
| Governing Body | The National Uniform Billing Committee (NUBC) oversees the UB-04 form and its standards. |
| Format | The form is structured in a specific format that includes various fields for patient and billing information. |
| Submission | Providers must submit the UB-04 form to insurance companies and government payers for reimbursement. |
| State-Specific Laws | Each state may have additional laws governing the use of the UB-04 form, including regulations on patient privacy and billing practices. |
| Data Elements | The form includes fields for patient demographics, service dates, and charges, among other details. |
| Certification | By submitting the UB-04, providers certify that the information is accurate and complete, which is crucial for compliance. |
Filling out the UB-04 form requires careful attention to detail, as it is essential for billing purposes in healthcare settings. This form captures various information about the patient, the services provided, and the billing details necessary for insurance claims. Once you have completed the form, it will be submitted to the appropriate payer for processing.
What is the UB-04 form?
The UB-04 form, also known as the CMS-1450, is a standardized billing form used by hospitals and other healthcare facilities to submit claims for services provided to patients. This form is essential for billing Medicare, Medicaid, and many private insurance companies. It contains detailed information about the patient, the services rendered, and the associated costs.
Who uses the UB-04 form?
The UB-04 form is primarily used by hospitals, skilled nursing facilities, and other healthcare providers. It is designed for institutional billing, meaning it is typically used for inpatient and outpatient services provided in a facility setting. Insurance companies and government programs rely on this form to process claims efficiently.
What information is required on the UB-04 form?
Several key pieces of information must be included on the UB-04 form. This includes the patient's name, address, date of birth, and insurance details. Additionally, the form requires information about the services provided, such as dates of service, procedure codes, and charges. Accurate and complete information is crucial for timely processing and payment of claims.
How do I fill out the UB-04 form?
Filling out the UB-04 form requires attention to detail. Start by entering patient information in the designated fields. Next, provide details about the services rendered, including revenue codes and descriptions. Be sure to include any applicable diagnosis codes and ensure that all information is accurate. It may be helpful to refer to the instructions provided by the National Uniform Billing Committee for guidance.
What happens if there is an error on the UB-04 form?
Errors on the UB-04 form can lead to delays in payment or claim denials. If a mistake is discovered after submission, it is important to correct it as soon as possible. You may need to resubmit the claim with the correct information. Keeping thorough records can help track any issues and ensure that claims are processed smoothly.
How is the UB-04 form submitted?
The UB-04 form can be submitted electronically or in paper format, depending on the requirements of the payer. Many healthcare facilities prefer electronic submission for efficiency. If submitting by mail, ensure that the form is printed clearly and that all required fields are completed. Check with the specific insurance provider for their submission guidelines.
What are the consequences of misrepresenting information on the UB-04 form?
Misrepresentation or falsification of information on the UB-04 form can lead to serious consequences. This includes potential civil monetary penalties and criminal charges under federal or state laws. It is crucial to ensure that all information provided is accurate and truthful to avoid legal repercussions.
Where can I find more information about the UB-04 form?
For more detailed information about the UB-04 form, including data elements and printing specifications, you can visit the National Uniform Billing Committee's website. This resource provides comprehensive guidance and updates related to the form and its use in healthcare billing.
Incomplete Patient Information: Failing to provide complete details such as the patient's name, address, and birthdate can lead to significant delays in processing claims.
Incorrect Coding: Using the wrong codes for diagnoses or procedures can result in denied claims. It's essential to verify that the codes align with the services rendered.
Missing Signature: Not obtaining the necessary signatures for authorization can cause the claim to be rejected. Ensure that the patient or their representative has signed where required.
Wrong Dates: Entering incorrect service dates can lead to confusion and claims being denied. Double-check all date entries for accuracy.
Ignoring Payer Requirements: Different insurance companies have specific requirements. Not adhering to these can result in claim denials. Always review the payer’s guidelines.
Failure to Document Supporting Information: Not including necessary documentation, such as medical necessity letters or prior authorizations, can jeopardize the claim. Maintain thorough records to support the claim.
The UB-04 form, also known as the CMS-1450, is a critical document used for billing healthcare services provided to patients in institutional settings. Along with the UB-04, several other forms and documents are often utilized to ensure accurate billing and compliance with regulations. Here is a list of commonly associated documents:
These documents work together to create a comprehensive billing process that ensures accuracy, compliance, and clear communication between healthcare providers, patients, and insurers. Understanding the role of each form can significantly enhance the efficiency of healthcare billing and claims management.
The CMS-1500 form is a key document in the medical billing process, similar to the UB-04 form. While the UB-04 is primarily used by institutional providers, such as hospitals and skilled nursing facilities, the CMS-1500 is designed for individual healthcare providers, including physicians and therapists. Both forms serve the purpose of submitting claims to insurance companies for reimbursement of medical services rendered. They require detailed information about the patient, the services provided, and the billing codes that correspond to those services. The CMS-1500 form focuses more on outpatient services, whereas the UB-04 is tailored for inpatient and facility-based claims.
The HCFA 1450 form, now known as the UB-04, shares similarities in its purpose and structure. Originally, the HCFA 1450 was the standard claim form for institutional providers before the UB-04 was introduced. Both forms require similar data elements, such as patient demographics, billing codes, and service dates. The transition from HCFA 1450 to UB-04 aimed to streamline the billing process and improve the accuracy of claims submissions. Although the UB-04 has become the standard, understanding the HCFA 1450 is essential for those who may encounter older billing systems or records.
The ANSI X12 837 Institutional transaction is another document that parallels the UB-04 form. This electronic format is used for submitting healthcare claims to payers in a standardized way. Just like the UB-04, the ANSI X12 837 includes comprehensive information about the patient, services provided, and the associated billing codes. The key difference lies in the format; the UB-04 is a paper form, while the ANSI X12 837 is an electronic submission. Both aim to ensure that healthcare providers receive timely and accurate reimbursement for services rendered.
The Medicare Summary Notice (MSN) also bears resemblance to the UB-04, though it serves a different purpose. The MSN is a document that patients receive after their healthcare services have been processed by Medicare. It summarizes the services provided, the amount billed, and the amount covered by Medicare, along with any patient responsibility. While the UB-04 is used to submit claims, the MSN is the result of that submission, providing transparency to patients about their healthcare costs. Both documents play crucial roles in the healthcare billing cycle, ensuring that providers are paid and patients understand their financial obligations.
When filling out the UB-04 form, accuracy and attention to detail are crucial. Here are five essential do's and don'ts to keep in mind:
When it comes to the UB-04 form, misconceptions can lead to confusion and errors in billing. Here are nine common misconceptions about this important document, along with clarifications to help you understand its purpose better.
By addressing these misconceptions, you can navigate the complexities of healthcare billing more effectively. Understanding the UB-04 form will help ensure accurate submissions and timely payments.
Filling out and using the UB-04 form requires careful attention to detail. Here are key takeaways to consider:
These takeaways highlight the importance of diligence when completing the UB-04 form to facilitate proper billing and compliance with regulations.