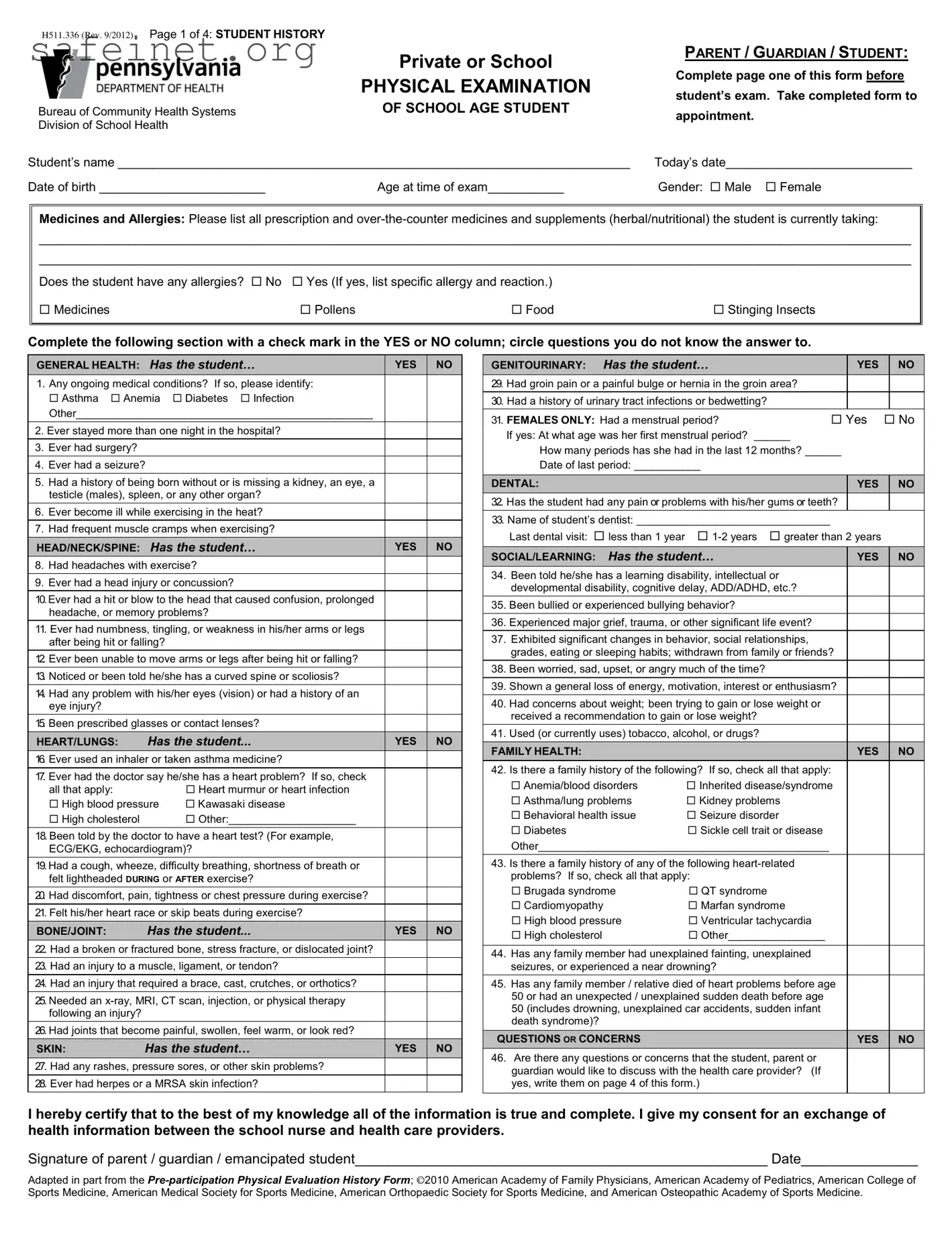
The Physical Exam form serves as an essential tool for assessing the health and well-being of school-age students. It captures vital information about the student’s medical history, including any ongoing conditions, allergies, and medications. Parents or guardians complete the first page, which features questions covering general health, heart and lung issues, and bone and joint conditions. This portion ensures that the healthcare provider has a comprehensive understanding of any potential concerns before the examination begins. Additionally, specific sections address social and learning aspects, such as any history of bullying or mental health issues, which can impact a student's overall development. The second page of the form is dedicated to the actual physical examination details, where the healthcare provider records observations related to height, weight, and general physical condition. Immunization history is crucial as well, ensuring compliance with health regulations while helping to protect the community. By filling out this form, parents and guardians actively contribute to the health and safety of their children, facilitating open communication between families and healthcare providers.
H511.336 (Rev. 9/2012) Page 1 of 4: STUDENT HISTORY
|
Private or School |
|
PHYSICAL EXAMINATION |
Bureau of Community Health Systems |
OF SCHOOL AGE STUDENT |
Division of School Health |
|
Student’s name __________________________________________________________________________
Date of birth ________________________ |
Age at time of exam___________ |
PARENT / GUARDIAN / STUDENT:
Complete page one of this form before student’s exam. Take completed form to
appointment.
Today’s date___________________________
Gender: Male Female
Medicines and Allergies: Please list all prescription and
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
Does the student have any allergies? No Yes (If yes, list specific allergy and reaction.)
Medicines |
Pollens |
Food |
Stinging Insects |
|
|
|
|
Complete the following section with a check mark in the YES or NO column; circle questions you do not know the answer to.
|
GENERAL HEALTH: Has the student… |
|
|
|
|
||
|
|
YES |
|
NO |
|||
|
1. Any ongoing medical conditions? If so, please identify: |
|
|
|
|
||
|
Asthma Anemia |
Diabetes Infection |
|
|
|
|
|
|
Other_________________________________________________ |
|
|
|
|
||
|
|
|
|
|
|||
2. Ever stayed more than one night in the hospital? |
|
|
|
|
|||
|
|
|
|
|
|
|
|
3. Ever had surgery? |
|
|
|
|
|
|
|
4. Ever had a seizure? |
|
|
|
|
|
||
|
|
|
|
|
|||
5. Had a history of being born without or is missing a kidney, an eye, a |
|
|
|
|
|||
|
testicle (males), spleen, or any other organ? |
|
|
|
|
||
6. Ever become ill while exercising in the heat? |
|
|
|
|
|||
7. Had frequent muscle cramps when exercising? |
|
|
|
|
|||
|
|
|
|
|
|
||
|
HEAD/NECK/SPINE: Has the student… |
|
YES |
|
NO |
||
8. Had headaches with exercise? |
|
|
|
|
|||
|
|
|
|
|
|||
9. Ever had a head injury or concussion? |
|
|
|
|
|||
|
|
|
|
|
|||
10.Ever had a hit or blow to the head that caused confusion, prolonged |
|
|
|
|
|||
|
headache, or memory problems? |
|
|
|
|
||
11. Ever had numbness, tingling, or weakness in his/her arms or legs |
|
|
|
|
|||
|
after being hit or falling? |
|
|
|
|
|
|
|
|
|
|
|
|||
12. Ever been unable to move arms or legs after being hit or falling? |
|
|
|
|
|||
13. Noticed or been told he/she has a curved spine or scoliosis? |
|
|
|
|
|||
|
|
|
|
|
|||
14. Had any problem with his/her eyes (vision) or had a history of an |
|
|
|
|
|||
|
eye injury? |
|
|
|
|
|
|
15. Been prescribed glasses or contact lenses? |
|
|
|
|
|||
|
HEART/LUNGS: |
Has the student... |
|
YES |
|
NO |
|
16. Ever used an inhaler or taken asthma medicine? |
|
|
|
|
|||
17. Ever had the doctor say he/she has a heart problem? If so, check |
|
|
|
|
|||
|
all that apply: |
|
Heart murmur or heart infection |
|
|
|
|
|
High blood pressure |
Kawasaki disease |
|
|
|
|
|
|
High cholesterol |
|
Other:_____________________ |
|
|
|
|
18. Been told by the doctor to have a heart test? (For example, |
|
|
|
|
|||
|
ECG/EKG, echocardiogram)? |
|
|
|
|
||
|
|
|
|
|
|||
19.Had a cough, wheeze, difficulty breathing, shortness of breath or |
|
|
|
|
|||
|
felt lightheaded DURING or AFTER exercise? |
|
|
|
|
||
|
|
|
|
|
|||
20. Had discomfort, pain, tightness or chest pressure during exercise? |
|
|
|
|
|||
|
|
|
|
|
|||
21. Felt his/her heart race or skip beats during exercise? |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
BONE/JOINT: |
Has the student... |
|
YES |
|
NO |
|
22. Had a broken or fractured bone, stress fracture, or dislocated joint? |
|
|
|
|
|||
|
|
|
|
|
|||
23. Had an injury to a muscle, ligament, or tendon? |
|
|
|
|
|||
24. Had an injury that required a brace, cast, crutches, or orthotics? |
|
|
|
|
|||
|
|
|
|
|
|||
25. Needed an |
|
|
|
|
|||
|
following an injury? |
|
|
|
|
|
|
|
|
|
|
|
|||
26. Had joints that become painful, swollen, feel warm, or look red? |
|
|
|
|
|||
|
SKIN: |
Has the student… |
|
YES |
|
NO |
|
27. Had any rashes, pressure sores, or other skin problems? |
|
|
|
|
|||
28. Ever had herpes or a MRSA skin infection? |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
Has the student… |
|
|
|
|
|
|
|
|
||
|
GENITOURINARY: |
|
|
YES |
|
|
|
NO |
|
|||
|
29. Had groin pain or a painful bulge or hernia in the groin area? |
|
|
|
|
|
|
|
|
|||
|
30. Had a history of urinary tract infections or bedwetting? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|||||||
|
31. FEMALES ONLY: Had a menstrual period? |
Yes |
No |
|||||||||
|
|
If yes: At what age was her first menstrual period? ______ |
|
|
|
|
|
|
|
|
||
|
|
How many periods has she had in the last 12 months? ______ |
|
|
|
|
||||||
|
|
Date of last period: ___________ |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
DENTAL: |
|
|
|
|
YES |
|
|
NO |
|||
|
32. Has the student had any pain or problems with his/her gums or teeth? |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
33. Name of student’s dentist: ________________________________ |
|
|
|
|
|
|
|
|
|||
|
|
Last dental visit: less than 1 year |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||||
|
SOCIAL/LEARNING: |
Has the student… |
|
|
YES |
|
|
NO |
||||
34. |
Been told he/she has a learning disability, intellectual or |
|
|
|
|
|
|
|
|
|||
|
|
developmental disability, cognitive delay, ADD/ADHD, etc.? |
|
|
|
|
|
|
|
|
||
35. |
Been bullied or experienced bullying behavior? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
36. |
Experienced major grief, trauma, or other significant life event? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
37. |
Exhibited significant changes in behavior, social relationships, |
|
|
|
|
|
|
|
|
|||
|
|
grades, eating or sleeping habits; withdrawn from family or friends? |
|
|
|
|
|
|||||
38. |
Been worried, sad, upset, or angry much of the time? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
||||||
39. |
Shown a general loss of energy, motivation, interest or enthusiasm? |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
40. |
Had concerns about weight; been trying to gain or lose weight or |
|
|
|
|
|
|
|
|
|||
|
|
received a recommendation to gain or lose weight? |
|
|
|
|
|
|
|
|
||
41. |
Used (or currently uses) tobacco, alcohol, or drugs? |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
FAMILY HEALTH: |
|
|
|
|
YES |
|
|
|
NO |
|
|
42. |
Is there a family history of the following? If so, check all that apply: |
|
|
|
|
|
|
|
|
|||
|
|
Anemia/blood disorders |
Inherited disease/syndrome |
|
|
|
|
|
||||
|
|
Asthma/lung problems |
Kidney problems |
|
|
|
|
|
|
|
|
|
|
|
Behavioral health issue |
Seizure disorder |
|
|
|
|
|
|
|
|
|
|
|
Diabetes |
|
Sickle cell trait or disease |
|
|
|
|
|
|
|
|
|
Other________________________________________________ |
|
|
|
|
|
|
|
|
|||
43. |
Is there a family history of any of the following |
|
|
|
|
|
|
|
|
|||
|
|
problems? If so, check all that apply: |
|
|
|
|
|
|
|
|
||
|
Brugada syndrome |
QT syndrome |
|
|
|
|
|
|
|
|
||
|
|
Cardiomyopathy |
|
Marfan syndrome |
|
|
|
|
|
|
|
|
|
|
High blood pressure |
Ventricular tachycardia |
|
|
|
|
|
|
|
|
|
|
|
High cholesterol |
|
Other________________ |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
44. |
Has any family member had unexplained fainting, unexplained |
|
|
|
|
|
|
|
|
|||
|
|
seizures, or experienced a near drowning? |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||||||
45. |
Has any family member / relative died of heart problems before age |
|
|
|
|
|
||||||
|
|
50 or had an unexpected / unexplained sudden death before age |
|
|
|
|
|
|
|
|
||
|
|
50 (includes drowning, unexplained car accidents, sudden infant |
|
|
|
|
|
|
|
|
||
|
|
death syndrome)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
QUESTIONS OR CONCERNS |
|
|
|
YES |
|
|
|
NO |
|
||
46. |
Are there any questions or concerns that the student, parent or |
|
|
|
|
|
|
|
|
|||
|
|
guardian would like to discuss with the health care provider? (If |
|
|
|
|
|
|
|
|
||
|
|
yes, write them on page 4 of this form.) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
I hereby certify that to the best of my knowledge all of the information is true and complete. I give my consent for an exchange of health information between the school nurse and health care providers.
Signature of parent / guardian / emancipated student_____________________________________________________ Date_______________
Adapted in part from the
Page 2 of 4: PHYSICAL EXAM
STUDENT’S HEALTH HISTORY (page 1 of this form) REVIEWED PRIOR TO PERFOMING EXAMINATION: Yes |
No |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CHECK ONE |
|
|
|
||
Physical exam for grade: |
|
|
|
|
|
|
|
|||
|
NORMAL |
*ABNORMAL |
DEFER |
|
|
|
||||
K/1 6 11 |
Other |
*ABNORMAL FINDINGS / RECOMMENDATIONS / REFERRALS |
|
|||||||
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
Height: |
( |
|
) inches |
|
|
|
|
|
|
|
Weight: |
( |
|
) pounds |
|
|
|
|
|
|
|
BMI: |
( |
|
) |
|
|
|
|
|
|
|
|
) % |
|
|
|
|
|
|
|||
Pulse: |
( |
|
) |
|
|
|
|
|
|
|
Blood Pressure: |
( |
/ |
) |
|
|
|
|
|
|
|
Hair/Scalp |
|
|
|
|
|
|
|
|
|
|
Skin |
|
|
|
|
|
|
|
|
|
|
Eyes/Vision |
Corrected |
|
|
|
|
|
|
|||
Ears/Hearing |
|
|
|
|
|
|
|
|
|
|
Nose and Throat |
|
|
|
|
|
|
|
|
|
|
Teeth and Gingiva |
|
|
|
|
|
|
|
|
||
Lymph Glands |
|
|
|
|
|
|
|
|
|
|
Heart |
|
|
|
|
|
|
|
|
|
|
Lungs |
|
|
|
|
|
|
|
|
|
|
Abdomen |
|
|
|
|
|
|
|
|
|
|
Genitourinary |
|
|
|
|
|
|
|
|
|
|
Neuromuscular System |
|
|
|
|
|
|
|
|
||
Extremities |
|
|
|
|
|
|
|
|
|
|
Spine (Scoliosis) |
|
|
|
|
|
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
TUBERCULIN TEST |
DATE APPLIED |
|
|
DATE READ
MEDICAL CONDITIONS OR CHRONIC DISEASES WHICH REQUIRE MEDICATION, RESTRICTION OF ACTIVITY, OR WHICH MAY AFFECT EDUCATION
(Additional space on page 4)
Parent/guardian present during exam: Yes |
No |
|
|
Physical exam performed at: Personal Health Care Provider’s Office |
School |
Date of exam______________20______ |
|
Print name of examiner _______________________________________________________________________________________________________
Print examiner’s office address___________________________________________________________________ Phone_______________________
Signature of examiner______________________________________________________________________ MD DO PAC CRNP
Page 3 of 4: IMMUNIZATION HISTORY
HEALTH CARE PROVIDERS: Please photocopy immunization history from student’s record – OR – insert information below.
IMMUNIZATION EXEMPTION(S):
Medical |
Date Issued:___________ |
Reason: __________________________________________________ |
Date Rescinded:___________ |
Medical |
Date Issued:___________ |
Reason: __________________________________________________ |
Date Rescinded:___________ |
Medical |
Date Issued:___________ |
Reason: __________________________________________________ |
Date Rescinded:___________ |
NOTE: The parent/guardian must provide a written request to the school for a religious or philosophical exemption.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VACCINE |
|
|
|
DOCUMENT: (1) Type of vaccine; (2) Date (month/day/year) for each immunization |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Diphtheria/Tetanus/Pertussis (child) |
|
|
|
|
|
|
|
|
|
||
|
Type: DTaP, DTP or DT |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diphtheria/Tetanus/Pertussis |
|
1 |
|
2 |
3 |
4 |
5 |
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
(adolescent/adult) |
|
|
|
|
|
|
|
|
|
|
|
|
Type: Tdap or Td |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Polio |
|
|
|
|
|
|
|
|
|
|
|
|
Type: OPV or IPV |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Hepatitis B |
(HepB) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Measles/Mumps/Rubella (MMR) |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||
|
Mumps disease diagnosed by physician |
|
|
Date:__________ |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Varicella: |
Vaccine |
Disease |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Serology: (Identify Antigen/Date/POS or NEG) |
|
|
|
|
|
|
|
|
|
||
|
i.e. Hep B, Measles, Rubella, Varicella |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Meningococcal Conjugate Vaccine (MCV4) |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Human Papilloma Virus (HPV) |
|
|
|
|
|
|
|
|
|
||
|
Type: HPV2 or HPV4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Influenza |
|
|
|
6 |
|
7 |
8 |
9 |
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type: TIV (injected) |
|
|
|
|
|
|
|
|
|
|
|
|
LAIV (nasal) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
12 |
13 |
14 |
15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Haemophilus Influenzae Type b (Hib) |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Pneumococcal Conjugate Vaccine (PCV) |
|
|
|
|
|
|
|
|
|
||
|
Type: 7 or 13 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Hepatitis A (HepA) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
5 |
|
|
|
Rotavirus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other Vaccines: (Type and Date)
Page 4 of 4: ADDITIONAL COMMENTS (PARENT / GUARDIAN / STUDENT / HEALTH CARE PROVIDER)
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Physical Exam form is designed to collect crucial health-related information about school-aged students, necessary for participation in school activities. |
| Scope of Information | This form covers various health aspects, including medical history, allergies, medications, and social/learning concerns to provide a comprehensive view of the student’s health. |
| Legal Compliance | In most states, the use of the Physical Exam form aligns with laws governing school health assessments, ensuring that schools collect necessary health data for their students. |
| Required Signatures | A parent, guardian, or emancipated student must sign the form to certify the accuracy of the information provided and grant consent for information sharing with health care providers. |
| Immunization History Component | The form requires documentation of the student’s immunization history, highlighting the importance of vaccinations for public health and school attendance. |
| Gender Information | Students are required to indicate their gender on the form, which may assist in tailored health assessments and screenings. |
| Physical Health Indicators | The form includes sections to record vital medical indicators such as height, weight, and blood pressure, which are essential for evaluating the student’s overall health. |
| Confidentiality of Information | All information collected on the Physical Exam form is confidential and should be treated with respect to privacy laws, ensuring the student’s health information is protected. |
| Adaptation and Guidelines | This form is adapted in part from guidelines provided by reputable organizations such as the American Academy of Family Physicians, ensuring its relevance and accuracy. |
| State-Specific Variations | Different states may have additional requirements or variations to the Physical Exam form in accordance with local governing laws, such as immunization requirements and health screenings. |
Completing the Physical Exam form is essential for ensuring that all relevant health information is collected before the student’s examination. The following steps will guide you through filling out the form accurately and completely.
What is the purpose of the Physical Exam form?
The Physical Exam form is designed to gather important health information about a student before their examination. It allows parents or guardians to provide details about the child's medical history, current medications, allergies, and social or learning concerns. This information helps healthcare providers assess the student's health and identify any specific needs during the exam.
Who is responsible for completing the form?
The form should be completed by the parent, guardian, or emancipated student. They need to fill out the first page before the student's health appointment. It’s important to provide as much accurate information as possible to ensure the healthcare provider understands the student’s health history.
What information is required in the “Medicines and Allergies” section?
This section asks for a list of all prescription and over-the-counter medications, supplements, or herbal/nutritional products the student is currently taking. Additionally, it inquires about any known allergies the student may have, including the type of allergy and the reaction experienced. Filling this out helps avoid any potential adverse reactions during the examination.
Why is the student’s health history important?
The health history is crucial because it provides context for the physical exam. By reviewing the student's past medical conditions, surgeries, and injuries, the healthcare provider can better anticipate and address the student’s health needs during the examination. It can also guide decisions related to sports participation and other activities.
What happens if something is marked as “abnormal” on the form?
If any portion of the Physical Exam form indicates an abnormal finding, the healthcare provider will typically discuss these concerns with the parent or guardian. They may recommend further tests or referrals to ensure the student's health is appropriately monitored and managed.
Is it necessary to keep the information in the form updated?
Yes, it's vital to keep the information current. If there are any changes in the student’s health, medications, or allergies after the physical exam, those details should be updated in the student’s health records. This ensures all healthcare providers involved are aware of the student's latest health status and can provide appropriate care.
How is the Physical Exam form used by the school?
Once completed, the Physical Exam form is submitted to the school nurse and is kept on file. It helps the school monitor the health and wellbeing of students. The information can also assist in making decisions regarding health needs, accommodations, or interventions at school, especially for students with ongoing health concerns.
Leaving Sections Blank: It's crucial to fill out every relevant section of the form. If a question does not apply, indicate so instead of skipping it altogether. This helps the healthcare provider understand the student's complete background.
Not Including Current Medications: Students often fail to list all prescription and over-the-counter medications. Not disclosing current medications can lead to oversights during the physical exam or treatment recommendations.
Ignoring Allergies: If the student has allergies, it’s important to specify these, including the reactions they cause. Omitting allergies can place the student at risk, particularly during medical procedures.
Misunderstanding Medical History: Sometimes parents or guardians do not fully grasp the implications of medical history questions. Each question pertains to significant health information, which should be answered accurately.
Forgetting Family Health History: Family health history is a vital part of understanding potential genetic conditions. Not listing this information can lead to missed opportunities for preventative care.
Omitting Behavioral or Emotional Concerns: Issues like bullying or shifts in behavior should be documented. These factors can impact a child’s health and overall school performance and should not be overlooked.
Not Signing the Form: All parties listed on the form must ensure it is signed. A lack of signature can lead to complications in the treatment or the verification of information provided.
When preparing for a physical exam, several important documents may be required alongside the Physical Exam form. Each serves a different purpose in ensuring that the student's health is thoroughly evaluated and supported by necessary background information. Below are some of the frequently used documents:
Having these documents prepared can streamline the physical exam process and help ensure that all pertinent health information is readily available to healthcare providers. This thorough preparation plays a critical role in promoting the well-being of students.
The Physical Exam form shares similarities with the Medical History Questionnaire, which is often used in healthcare settings to gather background information about a patient’s health. Like the Physical Exam form, this questionnaire includes sections for personal details and medical history, such as allergies, ongoing medical conditions, and past hospital stays. This document also prioritizes input from both the patient and their caregiver, as accurate and comprehensive information is vital for effective healthcare assessments.
Another document similar to the Physical Exam form is the Consent for Treatment form. Typically required before any medical procedure, this form seeks permission from the parent or guardian for their child's medical evaluation or treatment. Both forms emphasize the importance of informed consent and often require signatures from caregivers, highlighting the need for trust and communication in the healthcare process.
The Immunization Record is yet another document that aligns closely with the Physical Exam form. This record details a student’s vaccination history, including dates and types of vaccinations received. Just as the Physical Exam form collects vital health information and alerts healthcare providers about potential issues, the Immunization Record ensures that students are up-to-date with required vaccines, protecting both individual and public health.
Lastly, the Health Assessment form also resembles the Physical Exam form in its purpose of gathering comprehensive health information. Used in various settings such as schools or camps, this document details a student’s physical condition, health history, and any necessary accommodations. Both forms cover similar topics, including family health history and current medications, guiding healthcare providers in making informed decisions regarding the student’s wellbeing.
When filling out the Physical Exam form, following certain guidelines can ensure accurate and comprehensive information is provided. Here are key do's and don'ts:
Misconceptions surrounding the Physical Exam form can lead to confusion and undermine its effectiveness. Understanding these misconceptions is crucial for parents, guardians, and students alike. Here’s a clear look at six common misconceptions:
Recognizing these misconceptions can help everyone involved ensure that the Physical Exam form serves its purpose effectively, promoting student health and readiness for school.
Filling out the Physical Exam form is essential for ensuring that a student receives appropriate health evaluations. Here are some key takeaways to consider: