The NJSP S.T.S. 033 form plays a crucial role in the regulatory landscape of New Jersey, particularly concerning the ownership and transfer of firearms. This document is essential for individuals seeking to apply for a permit to purchase a handgun or a firearms identification card. It encapsulates various aspects, such as the applicant's personal information, the nature of the firearm purchase, and the requisite background checks mandated by state law. The form serves not only as a means to ensure compliance with New Jersey's stringent firearm regulations but also as a protective measure for the community, aiming to prevent firearms from falling into the wrong hands. Furthermore, it embodies the state's commitment to upholding both the rights of responsible gun owners and the safety of its citizens. Completing the NJSP S.T.S. 033 requires thorough attention to detail, as any discrepancies may lead to delays or rejections of applications. Understanding the intricacies of this form is therefore vital for anyone navigating the process of firearm acquisition in New Jersey.
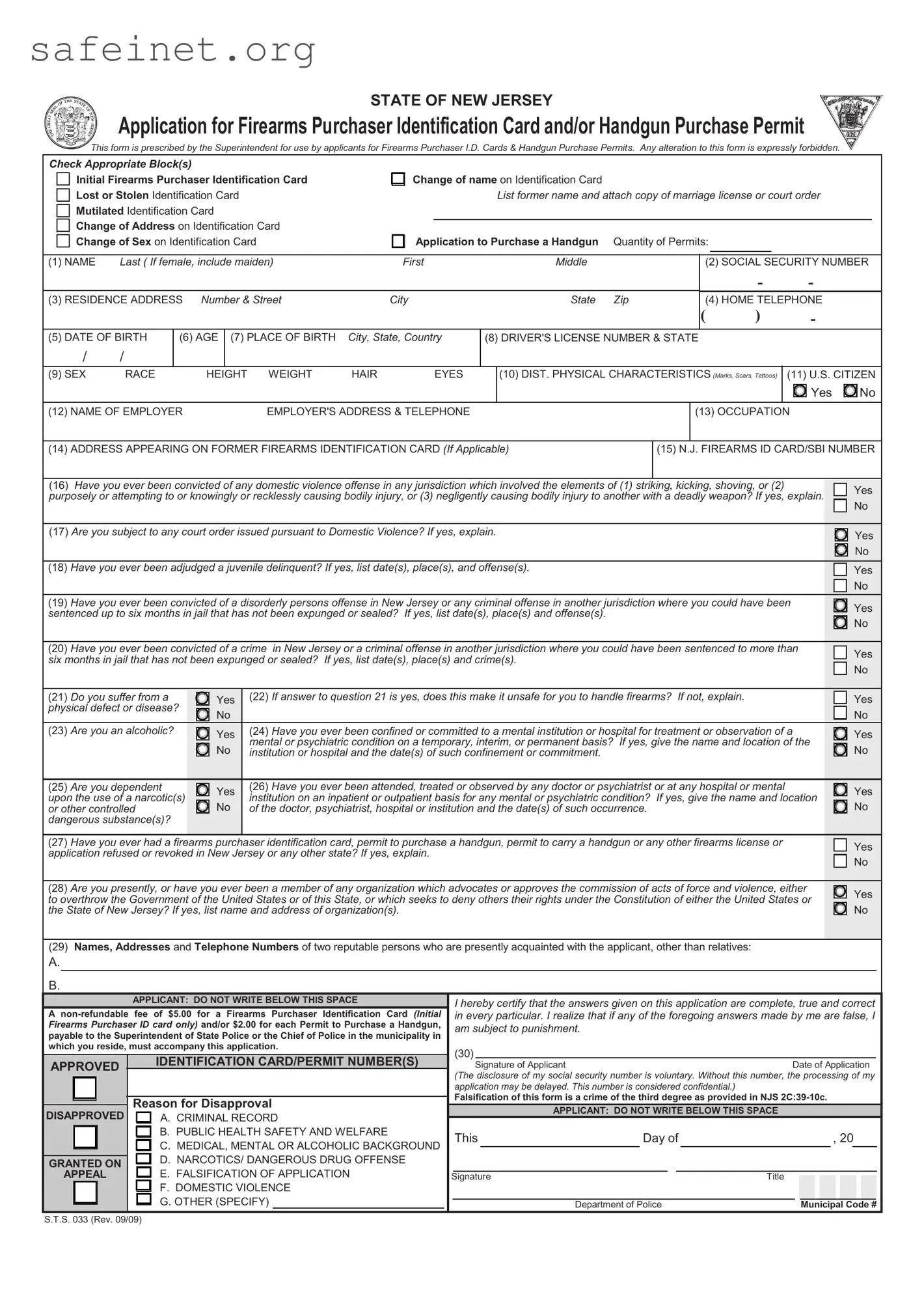
STATE OF NEW JERSEY
Application for Firearms Purchaser Identification Card and/or Handgun Purchase Permit
This form is prescribed by the Superintendent for use by applicants for Firearms Purchaser I.D. Cards & Handgun Purchase Permits. Any alteration to this form is expressly forbidden.
Check Appropriate Block(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Initial Firearms Purchaser Identification Card |
|
Change of name on Identification Card |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Lost or Stolen Identification Card |
|
|
|
|
|
List former name and attach copy of marriage license or court order |
|
|
|
||||||||||||||||||
Mutilated Identification Card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Change of Address on Identification Card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Change of Sex on Identification Card |
|
Application to Purchase a Handgun |
Quantity of Permits: |
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(1) NAME |
Last ( If female, include maiden) |
|
First |
|
Middle |
|
|
|
(2) SOCIAL SECURITY NUMBER |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
- |
|
|
|
|
(3) RESIDENCE ADDRESS |
Number & Street |
|
City |
|
State |
Zip |
|
|
(4) HOME TELEPHONE |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
|
) |
|
|
- |
|
|
|
|
(5) DATE OF BIRTH |
|
(6) AGE |
(7) PLACE OF BIRTH |
City, State, Country |
(8) DRIVER'S LICENSE NUMBER & STATE |
|
|
|
|
|
|
|
|
||||||||||||||
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(9) SEX |
RACE |
|
|
|
HEIGHT |
WEIGHT |
HAIR |
|
EYES |
|
(10) DIST. PHYSICAL CHARACTERISTICS (Marks, Scars, Tattoos) |
(11) U.S. CITIZEN |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
||
(12) NAME OF EMPLOYER |
|
|
|
|
EMPLOYER'S ADDRESS & TELEPHONE |
|
|
|
|
(13) OCCUPATION |
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
(14) ADDRESS APPEARING ON FORMER FIREARMS IDENTIFICATION CARD (If Applicable) |
|
(15) N.J. FIREARMS ID CARD/SBI NUMBER |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
(16) Have you ever been convicted of any domestic violence offense in any jurisdiction which involved the elements of (1) striking, kicking, shoving, or (2) |
|
|
|
Yes |
|||||||||||||||||||||||
purposely or attempting to or knowingly or recklessly causing bodily injury, or (3) negligently causing bodily injury to another with a deadly weapon? If yes, explain. |
|
|
|||||||||||||||||||||||||
|
|
No |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(17) Are you subject to any court order issued pursuant to Domestic Violence? If yes, explain. |
|
|
|
|
|
|
|
|
|
|
|
Yes |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
(18) Have you ever been adjudged a juvenile delinquent? If yes, list date(s), place(s), and offense(s). |
|
|
|
|
|
|
|
|
|
|
|
Yes |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
(19) Have you ever been convicted of a disorderly persons offense in New Jersey or any criminal offense in another jurisdiction where you could have been |
|
|
|
Yes |
|||||||||||||||||||||||
|
|
|
|||||||||||||||||||||||||
sentenced up to six months in jail that has not been expunged or sealed? If yes, list date(s), place(s) and offense(s). |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
No |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(20) Have you ever been convicted of a crime in New Jersey or a criminal offense in another jurisdiction where you could have been sentenced to more than |
|
|
|
Yes |
|||||||||||||||||||||||
six months in jail that has not been expunged or sealed? If yes, list date(s), place(s) and crime(s). |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
No |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(21) Do you suffer from a |
|
|
|
Yes |
|
(22) If answer to question 21 is yes, does this make it unsafe for you to handle firearms? If not, explain. |
|
|
|
|
|
|
Yes |
||||||||||||||
physical defect or disease? |
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
(23) Are you an alcoholic? |
|
|
|
Yes |
|
(24) Have you ever been confined or committed to a mental institution or hospital for treatment or observation of a |
|
|
|
Yes |
|||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
No |
|
mental or psychiatric condition on a temporary, interim, or permanent basis? If yes, give the name and location of the |
|
|
No |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
institution or hospital and the date(s) of such confinement or commitment. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
(25) Are you dependent |
|
|
|
Yes |
|
(26) Have you ever been attended, treated or observed by any doctor or psychiatrist or at any hospital or mental |
|
|
|
Yes |
|||||||||||||||||
upon the use of a narcotic(s) |
|
|
|
institution on an inpatient or outpatient basis for any mental or psychiatric condition? |
If yes, give the name and location |
|
|
||||||||||||||||||||
or other controlled |
|
|
|
No |
|
of the doctor, psychiatrist, hospital or institution and the date(s) of such occurrence. |
|
|
|
|
|
|
|
|
|
|
No |
||||||||||
dangerous substance(s)? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
(27) Have you ever had a firearms purchaser identification card, permit to purchase a handgun, permit to carry a handgun or any other firearms license or |
|
|
|
Yes |
|||||||||||||||||||||||
application refused or revoked in New Jersey or any other state? If yes, explain. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(28) Are you presently, or have you ever been a member of any organization which advocates or approves the commission of acts of force and violence, either |
|
|
|
Yes |
|||||||||||||||||||||||
to overthrow the Government of the United States or of this State, or which seeks to deny others their rights under the Constitution of either the United States or |
|
|
|||||||||||||||||||||||||
|
|
||||||||||||||||||||||||||
the State of New Jersey? If yes, list name and address of organization(s). |
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(29)Names, Addresses and Telephone Numbers of two reputable persons who are presently acquainted with the applicant, other than relatives:
A.
B.
|
|
|
|
APPLICANT: DO NOT WRITE BELOW THIS SPACE |
|
I hereby certify that the answers given on this application are complete, true and correct |
||||||||||||||||||||
A |
|
in every particular. I realize that if any of the foregoing answers made by me are false, I |
||||||||||||||||||||||||
Firearms Purchaser ID card only) and/or $2.00 for each Permit to Purchase a Handgun, |
|
am subject to punishment. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
payable to the Superintendent of State Police or the Chief of Police in the municipality in |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
which you reside, must accompany this application. |
(30) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
APPROVED |
IDENTIFICATION CARD/PERMIT NUMBER(S) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Signature of Applicant |
Date of Application |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
(The disclosure of my social security number is voluntary. Without this number, the processing of my |
||||||||||||||||||
|
|
|
|
|
|
|
|
application may be delayed. This number is considered confidential.) |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
Falsification of this form is a crime of the third degree as provided in NJS |
||||||||||||||||||
|
|
|
|
Reason for Disapproval |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
DISAPPROVED |
A. CRIMINAL RECORD |
|
|
|
|
APPLICANT: DO NOT WRITE BELOW THIS SPACE |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
B. PUBLIC HEALTH SAFETY AND WELFARE |
|
This |
|
Day of |
, 20 |
|
|
|
||||||||||||||
|
|
|
|
C. MEDICAL, MENTAL OR ALCOHOLIC BACKGROUND |
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
D. NARCOTICS/ DANGEROUS DRUG OFFENSE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
GRANTED ON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
APPEAL |
E. FALSIFICATION OF APPLICATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Signature |
|
|
|
|
|
Title |
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
F. DOMESTIC VIOLENCE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
G. OTHER (SPECIFY) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Department of Police |
|
|
Municipal Code # |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
S.T.S. 033 (Rev. 09/09)
| Fact Name | Description |
|---|---|
| Purpose of the Form | The NJSP S.T.S. 033 form is used to apply for a firearm purchaser identification card or a permit to purchase a handgun in New Jersey. |
| Governing Law | This form operates under the New Jersey Statutes Annotated (N.J.S.A.) 2C:58-3, which outlines the regulations for firearm purchases. |
| Eligibility Criteria | Applicants must be at least 18 years old, a resident of New Jersey, and must not have a felony conviction or a mental health disqualifier. |
| Application Process | Complete the form and submit it to the local police department or state police barracks along with the required identification and fees. |
| Approval Timeline | The law requires law enforcement to process the application within 30 days, barring any complications. |
| Renewal Requirements | Firearm purchaser identification cards do not expire, however, permits to purchase handguns are valid for only 90 days and cannot be renewed. |
| Record Keeping | Law enforcement agencies are required to keep records of all applications submitted through this form for a specific duration. |
After you have completed the NJSP S.T.S. 033 form, you will need to review it thoroughly to ensure all information is accurate and complete. Once verified, you can submit it to the appropriate agency following the specified submission guidelines. Whether you are applying for a permit or another purpose, proper completion is essential for processing your request efficiently.
What is the NJSP S.T.S. 033 form used for?
The NJSP S.T.S. 033 form is primarily used for background checks related to firearms purchases in New Jersey. This form is mandated by state law and ensures that applicants meet the necessary criteria to legally acquire a firearm. By completing this form, individuals provide essential personal information that helps law enforcement verify their eligibility.
Who needs to fill out the NJSP S.T.S. 033 form?
Anyone looking to purchase a firearm in New Jersey must complete the NJSP S.T.S. 033 form. This includes individuals applying for a handgun purchase permit or a firearm purchaser identification card. The form must be filled out correctly and submitted along with any required documentation to facilitate the background check process.
How do I submit the NJSP S.T.S. 033 form?
The NJSP S.T.S. 033 form can be submitted electronically through a designated system or in person at your local police department. After filling out the form, you may be required to provide identification and possibly other documents. It's important to follow the guidelines from your local law enforcement agency to ensure your application is processed smoothly.
What happens after I submit the NJSP S.T.S. 033 form?
Once you submit the NJSP S.T.S. 033 form, the local police department will conduct a background check. This process typically takes a few days. During this time, they will assess your criminal history, mental health status, and other relevant factors. You will be notified of the outcome, and if approved, you can proceed with your firearm purchase.
Failing to provide accurate personal information. Ensure that your name, address, and contact details are correct. Any discrepancies can lead to delays or denials.
Leaving sections blank. Every question on the form serves a purpose. It’s important to answer all questions fully, even if it means writing "not applicable" where necessary.
Omitting necessary documentation. Make sure to attach all required documents, such as identification and proof of residency. Missing documents can stall the review process.
Not reading the instructions carefully. Overlooking the guidelines can lead to mistakes. Take your time to understand what is being asked before filling out the form.
Using illegible handwriting. If you're filling the form out by hand, make sure your writing is clear and easy to read. Poor handwriting can result in misunderstandings.
Submitting the form late. Pay attention to deadlines. Late submissions may not be accepted, which could affect your application status.
Neglecting to review the form before submission. A final check can help catch mistakes or missing information. It’s always best to review everything carefully.
The NJSP S.T.S. 033 form is an important document often used in conjunction with various other forms and documents for the purposes of firearms applications, background checks, or permit requests in New Jersey. Below is a list of common forms that may accompany the NJSP S.T.S. 033 form, each serving a specific function within the application process.
Understanding and correctly compiling these documents is essential when filing an application alongside the NJSP S.T.S. 033 form. Each document serves a unique purpose and contributes to the overall assessment of the applicant’s qualifications for firearm ownership.
The NJSP S.T.S. 033 form is closely related to Form 4473, a crucial document used in the purchase of firearms in the United States. This federal form, required by the Bureau of Alcohol, Tobacco, Firearms and Explosives (ATF), mandates that an individual disclose personal information, background checks, and other details related to the purchase. Both forms serve to evaluate the eligibility of individuals seeking to acquire firearms, ensuring compliance with federal and state laws regarding firearm ownership. The information collected helps prevent firearms from falling into the hands of those who may pose a risk to society.
Another important document that shares similarities with the NJSP S.T.S. 033 form is the Application for a Firearms Identification Card (FID). This form is specific to New Jersey and is used for individuals seeking to own guns legally. Like the S.T.S. 033, the FID application requires extensive personal information, character references, and background checks. Both documents aim to ascertain the applicant’s suitability and dedication to responsible gun ownership, creating a regulatory framework for firearm transactions in the state.
The ATF Form 1, which is necessary for individuals or entities wanting to make or modify a firearm, also resembles the NJSP S.T.S. 033 form in purpose and required information. This form is part of the National Firearms Act (NFA) process and similarly necessitates personal identification, a detailed description of the firearm being modified, and an affirmation of eligibility. As with the NJSP S.T.S. 033, the intent is to regulate and track firearm-related activities, thereby promoting public safety through responsible practices.
The Concealed Carry Permit Application is another document that mirrors the function of the NJSP S.T.S. 033 form. This application process, which varies by state, often requires personal history, references, and proof of training. It aims to assess an applicant's fitness to carry a concealed weapon in public spaces. Like the S.T.S. 033, the concealed carry application emphasizes background checks and eligibility criteria, ensuring that only those deemed responsible citizens receive the right to carry firearms discreetly.
Lastly, the NICS Appeal Form holds a significant parallel to the NJSP S.T.S. 033 form. This form is utilized when a prospective gun buyer is denied the ability to purchase a firearm after a background check conducted through the National Instant Criminal Background Check System. Individuals can file this appeal if they believe the denial was made in error. Both forms serve as safeguards within the gun purchase process, facilitating a review of the applicant's eligibility while aiming to correct potential mistakes that may prevent law-abiding citizens from exercising their rights.
When filling out the NJSP S.T.S. 033 form, it is important to follow specific guidelines to ensure accuracy and compliance. Below is a list of things you should and shouldn't do during this process.
The NJSP S.T.S. 033 form can be surrounded by misunderstandings. Addressing these misconceptions can help clarify the process for those who need to complete this form.
Understanding these common misconceptions can lead to a smoother process when applying for a firearms purchaser ID card or handgun purchase permit in New Jersey.
When filling out and using the NJSP S.T.S. 033 form, it's important to follow the guidelines carefully. The following key takeaways can help ensure the process goes smoothly: