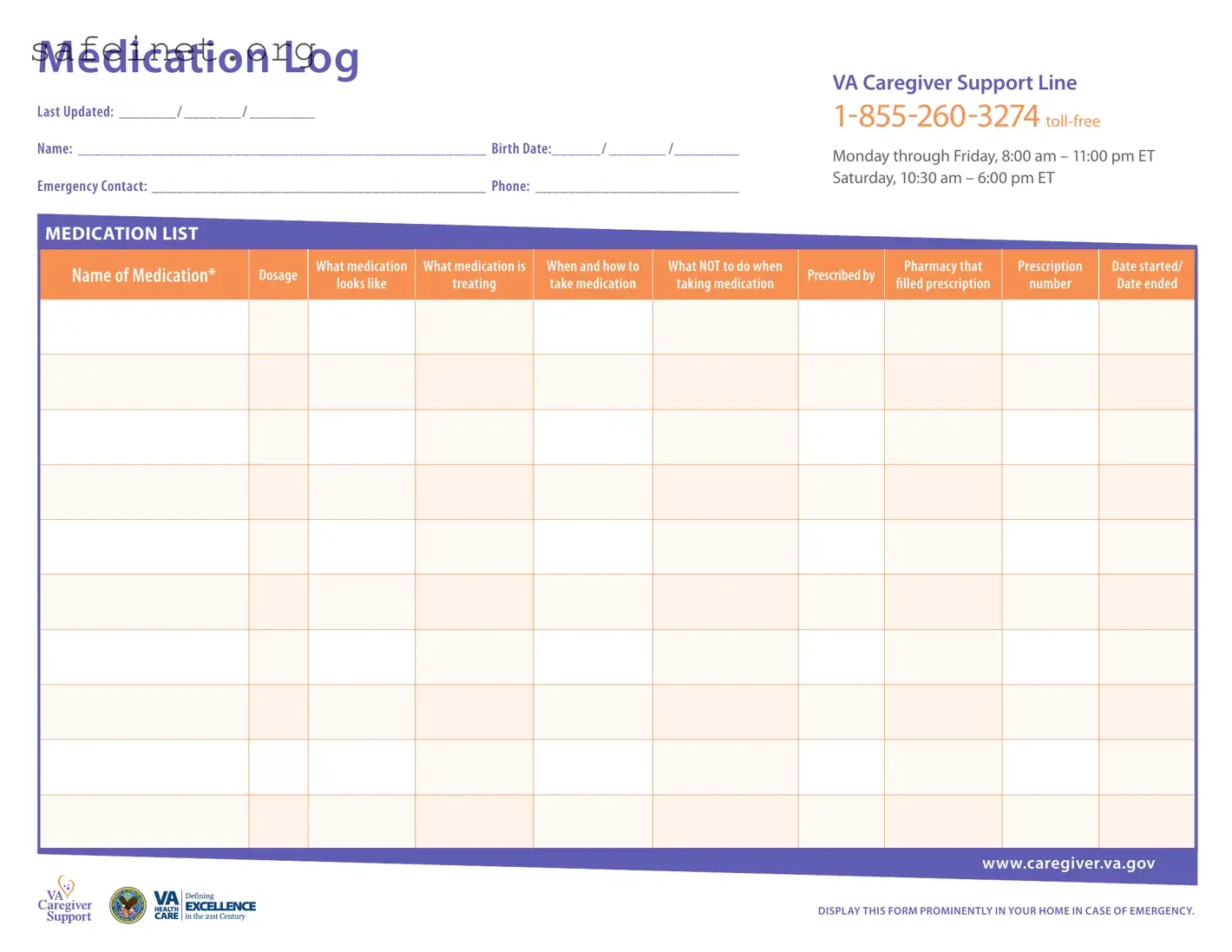
A Medication Log form serves as an essential tool for individuals managing medications, providing a clear and organized way to track pertinent information related to prescribed drugs. This form includes personal details such as the individual's name and birth date, along with emergency contact information and a direct line to the VA Caregiver Support Line, ensuring quick access to support if needed. A comprehensive medication list is the heart of the form, featuring columns to record the name, dosage, appearance, and purpose of each medication. It also specifies instructions on when and how to take the medication, as well as critical information on precautions to avoid while taking the medication. This log emphasizes the importance of recording the prescribing pharmacy and the prescription number, along with start and end dates for the treatment. To enhance safety, a section is dedicated to recording any drug allergies or significant reactions to medications, underscoring the need for awareness of potential side effects. For healthcare coordination, the form includes a section for listing primary care physicians and specialists, along with their contact information, further supporting effective communication among care providers. Finally, ample space is provided for notes, allowing caregivers and individuals to document any other relevant observations or concerns, reinforcing the overall goal of maintaining health and safety in medication management.

Medication Log
Last Updated: _______ / _______ / ________
Name: __________________________________________________ Birth Date:______ / _______ /________
Emergency Contact: _________________________________________ Phone: _________________________
VA Caregiver Support Line
Monday through Friday, 8:00 am – 11:00 pm ET Saturday, 10:30 am – 6:00 pm ET
MEDICATION LIST
Name of Medication*
Dosage
What medication
looks like
What medication is
treating
When and how to take medication
What NOT to do when
taking medication
Prescribed by
Pharmacy that
filled prescription
Prescription
number
Date started/
Date ended
www.caregiver.va.gov
DISPLAY THIS FORM PROMINENTLY IN YOUR HOME IN CASE OF EMERGENCY.
MEDICATION LIST
Name of Medication
Dosage
What medication |
What medication is |
When and how to |
looks like |
treating |
take medication |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
What NOT to do when
taking medication
Prescribed by
Pharmacy that
filled prescription
Prescription
number
Date started/
Date ended
www.caregiver.va.gov
Medication Log
REACTIONS
Drug Allergies and Other Signiicant Reactions
Prescription Name |
Reaction |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recent Medications that Caused Problems or Did Not Work
Prescription Name |
Problem |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHYSICIANS
Primary Care Physician
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
NOTES:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
REACTIONS
Drug Allergies and Other Signiicant Reactions
|
Prescription Name |
Reaction |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Recent Medications that Caused Problems or Did Not Work
Prescription Name |
Problem |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHYSICIANS
Primary Care Physician
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
Specialist
PHONE: |
ADDRESS: |
|
|
NOTES:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
| Fact Name | Description |
|---|---|
| Purpose | The Medication Log form serves to record all medications taken, ensuring that caregivers and medical professionals have quick access to essential information in emergencies. |
| Emergency Preparedness | Displaying the form prominently in the home is critical, as it allows emergency responders to quickly understand the medical history and current medications of the individual. |
| Legal Compliance | In many states, maintaining an updated Medication Log is mandatory under health care laws to ensure patient safety and proper medication management. |
| Pharmacy Information | The form requires details about pharmacy information and prescription numbers, facilitating efficient communication with pharmacists in case of emergencies. |
Completing the Medication Log form is essential for managing medications effectively and ensuring everyone involved in your care has access to the necessary information. Follow the steps below to accurately fill out the form.
This form serves as a comprehensive resource regarding your medications and medical contacts, facilitating prompt access in the event of an emergency. Display it prominently in your home for easy reference.
What is the purpose of the Medication Log form?
The Medication Log form serves as a comprehensive record of medications taken by an individual. It is designed to provide essential details about each medication, including dosage, appearance, and purpose. The form also outlines critical information regarding when and how to take the medication, as well as important warnings about what not to do while taking it. By keeping this log organized and updated, caregivers can ensure that medical professionals are fully informed about a patient's medication history, which is vital for their health and safety.
How should the Medication Log form be displayed?
It is recommended to display the Medication Log form prominently in your home. In case of an emergency, having easy access to this information can be crucial for medical responders. Consider placing it on the refrigerator or another central location where it can be quickly retrieved. Always ensure that anyone involved in the individual's care is aware of the form's location and its contents. This practice can significantly enhance safety and coordination of care.
What should I do if there are changes in medications?
If there are any changes to the medications—such as new prescriptions, dosage adjustments, or discontinued medications—it is important to update the Medication Log form immediately. Keeping this information current ensures that all caregivers and medical providers have access to the most accurate data, helping to prevent medication errors. Regular reviews of the form can aid in spotting any discrepancies or potential issues that may arise as treatment plans evolve.
What information should I include regarding drug allergies and reactions?
When completing the Medication Log form, be diligent about noting any drug allergies or significant reactions. This section should include the name of the medication that caused a reaction, the nature of that reaction, and the recent medications that may not have worked effectively. Accurate records of allergies and adverse reactions are critical in safeguarding the individual from future incidents and informing healthcare providers of any known sensitivities or historical challenges related to the person’s medication regimen.
Failing to update the date of the medication log can result in confusion. An incorrect date may lead to taking outdated medications.
Neglecting to provide full names of medications can create issues in emergencies. Abbreviations or nicknames may not be understood by health professionals.
Omitting the dosage can be dangerous. An inaccurate or missing dosage information could lead to administration mistakes.
Failing to include how and when to take the medication often leads to incorrect timing or inappropriate administration methods.
Ignoring the 'what NOT to do' section serves as a disservice. Not outlining contraindications may lead to potential adverse reactions.
Not writing down prescriber's information is another common error. Such details are crucial for direct communication regarding medication.
Inaccurate or missing pharmacy information can impede refills or address any issues that arise with prescriptions.
Lastly, failing to document drug allergies and significant reactions can pose serious health risks. Complete records are essential for safe medication management.
The Medication Log form is an essential tool for managing medication effectively and ensuring safety in medical care. However, it is often accompanied by several other important documents that enhance understanding, support communication, and establish a comprehensive health record. Below is a collection of forms that work harmoniously with the Medication Log, each playing a distinct role in the healthcare journey.
These forms collectively contribute to a thorough understanding of patient health, enhancing communication between all parties involved. By utilizing the Medication Log alongside these documents, caregivers and healthcare providers can ensure a safer and more efficient medication management process.
The Medication Administration Record (MAR) is similar to the Medication Log in that it is used for tracking medications a patient is prescribed. While the Medication Log serves as a master list for caregivers, the MAR is typically utilized in medical facilities to document each time a medication is administered. Clear and concise records of dosage, timing, and any reactions are maintained in the MAR, ensuring that healthcare providers can easily confirm what medication has been given to a patient and when.
The Patient Medication List provides a summary for individuals and families about what medications a patient is currently taking. Much like the Medication Log, this document includes crucial details like dosage and prescribed timing. However, it usually lacks the detailed sections for reactions and physician contact information that the Medication Log offers. The focus here is more on presenting a quick glance at all medications for easy reference, rather than a comprehensive tracking of administration and side effects.
The Prescription Record Document captures essential information when a prescription is filled. Similar to the Medication Log, it includes details about medication names and dosages. However, this document primarily focuses on the specifics related to the prescription process, such as the pharmacy where the prescription was filled and relevant dates. It lacks the ongoing treatment tracking elements found in the Medication Log, which is intended for active daily use.
The Allergy and Reaction Documentation is aligned with the Medication Log's section on drug allergies and other significant reactions. Both documents aim to keep a record of adverse drug reactions for patient safety. The main difference lies in the breadth of usage; while the Medication Log is comprehensive in detailing both current medications and reactions, allergy-specific documents may focus primarily on identifying potential allergens and past negative responses to medications, without prescribing information.
The Caregiver Instruction Sheet is another document that bears a resemblance to the Medication Log, designed to provide caregivers with essential information guiding patient care. This sheet often details how to administer medications properly and includes warning signs to watch for. While both documents cater to the needs of caregivers, the Instruction Sheet is more about “how to” care for a patient, whereas the Medication Log is a running registry of medications and related information.
The Clinical Assessment Form may also reflect similarities with the Medication Log. This document is often used to record a patient’s overall health status, including medication effects, side effects, and adjustments made during clinical visits. Both documents encourage the tracking of medication responses, but the Clinical Assessment Form is broader, addressing various aspects of a patient's health beyond just medications.
The Health History Questionnaire often resembles the structure of the Medication Log as it seeks to gather vital health information, including medications. While it may include questions regarding current medications, the focus is usually on past health issues, surgeries, and treatments. This document is essential for creating a comprehensive health profile but does not serve the same ongoing management purpose that the Medication Log provides.
The Discharge Summary is similar in purpose as it serves to communicate important medication information to both the patient and follow-up care providers once the patient leaves a healthcare facility. Both the Discharge Summary and the Medication Log aim to ensure continuity of care, providing essential details related to medications prescribed. However, the Discharge Summary is more of a one-time report while the Medication Log functions as a dynamic, ongoing document to be updated regularly.
When filling out the Medication Log form, keeping a few essential guidelines in mind can ensure accuracy and clarity. Here’s a helpful list of what to do and what to avoid.
Understanding the Medication Log form is crucial for anyone managing medication for themselves or a loved one. However, several misconceptions often lead to confusion. Here are six common misunderstandings:
While it is vital in emergencies, the Medication Log is also a useful tool for daily management. Having an organized record helps caregivers track medications and ensures they’re taken correctly.
Even with a single medication, using the log can provide clarity about dosages and timings. It also helps to note any side effects or reactions for future reference.
Filling out the log accurately is important. Anyone using it should understand the medications involved. Ideally, a healthcare provider or pharmacist should assist with this task.
Changes in medication, dosages, or prescribed treatments should always be documented promptly. This keeps the log current and useful for anyone referencing it.
The log can include over-the-counter medications and supplements, too. Capturing all substances taken can help healthcare providers understand the full picture of health.
This form can benefit anyone managing medications, including patients themselves. It encourages personal accountability and awareness of one’s treatment regimen.
By clearing up these misconceptions, users can maximize the benefits of maintaining a Medication Log and improve their medication management experience.
Keep the Medication Log updated regularly. This tool is essential for tracking medications accurately, and it should include the latest information on each prescription, including dosages and any changes in the regimen.
Display the Medication Log prominently in your home. In case of an emergency, having this important document easily accessible can assist medical personnel in providing the best care possible.
Note drug allergies and significant reactions clearly. This information helps prevent adverse reactions and ensures safer medication practices.
Designate a primary care physician and specialists on the log. Keeping their contact details readily available facilitates easier communication and coordination of care.