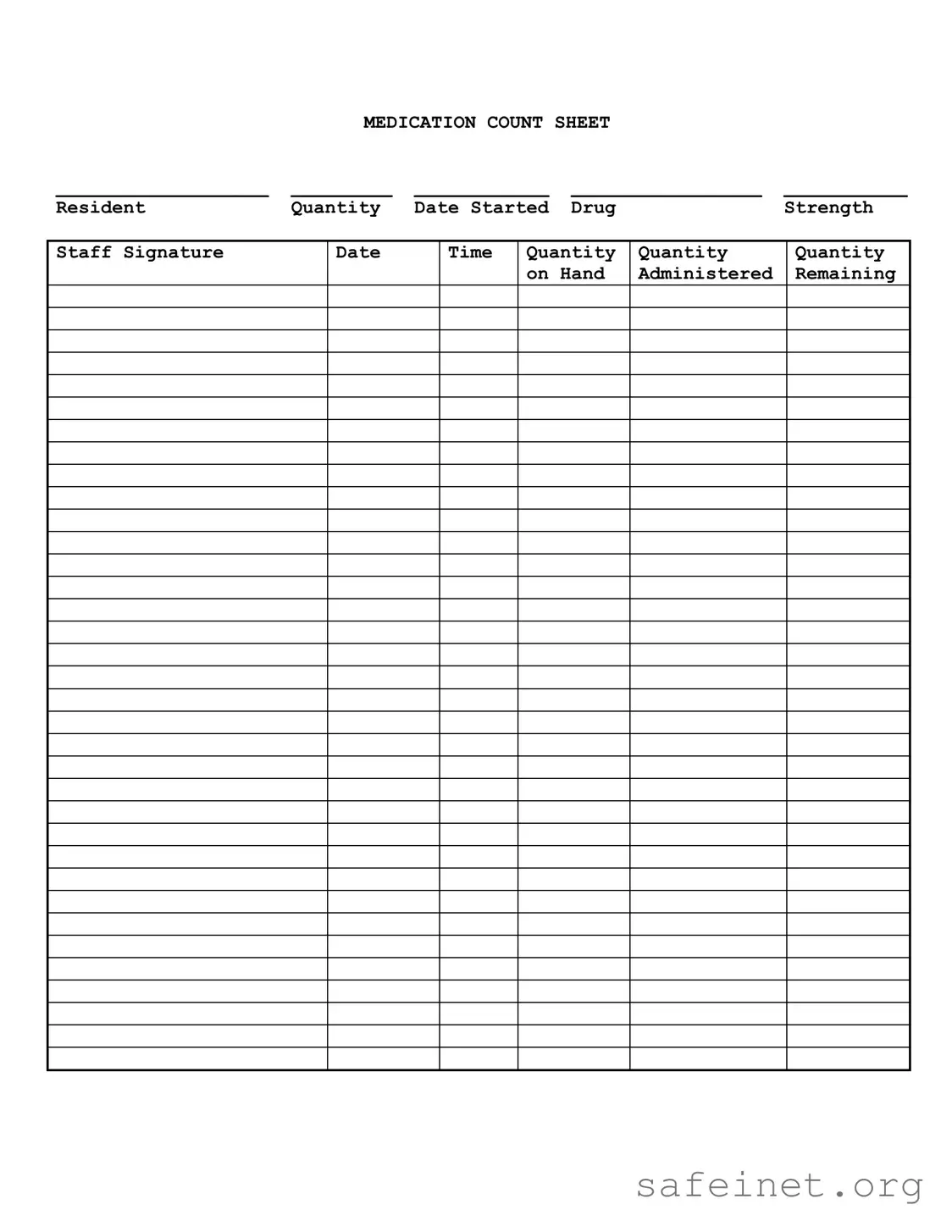
The Medication Count Sheet serves as a crucial tool in the management of medication within healthcare settings, ensuring accurate tracking and accountability of drug administration. This form typically includes essential details such as the resident's name, the quantity of medication, and the date the treatment began. Each entry also specifies the drug's strength, allowing staff to confirm the appropriate dosage is administered. Additionally, the Medication Count Sheet requires staff signatures to verify that medications have been given as prescribed, fostering transparency and responsibility. The form tracks the quantity administered, the quantity remaining, and the time of administration, creating a comprehensive record that aids in preventing errors and ensuring patient safety. By maintaining this detailed documentation, healthcare providers can uphold standards of care and enhance the overall effectiveness of medication management.
|
MEDICATION COUNT SHEET |
|
||
___________________ |
_________ |
____________ |
_________________ |
___________ |
Resident |
Quantity |
Date Started |
Drug |
Strength |
Staff Signature
Date
Time
Quantity |
Quantity |
Quantity |
on Hand |
Administered |
Remaining |
|
|
|
| Fact Name | Description |
|---|---|
| Purpose | The Medication Count Sheet is used to track the administration and inventory of medications for residents in care facilities. |
| Required Fields | Essential information includes the resident's name, drug strength, quantity on hand, and staff signature. |
| Frequency of Use | This sheet should be completed each time medication is administered to ensure accurate tracking. |
| State-Specific Forms | Some states require specific Medication Count Sheets governed by local regulations, such as the California Health and Safety Code. |
| Documentation | Accurate completion of the sheet serves as legal documentation of medication administration and inventory management. |
| Compliance | Failure to maintain an accurate Medication Count Sheet can lead to regulatory penalties and impact resident safety. |
Completing the Medication Count Sheet form is essential for maintaining accurate records of medication administration. Once filled out, this form will help ensure that medication is tracked properly, providing a clear account of what has been administered and what remains on hand.
What is the purpose of the Medication Count Sheet?
The Medication Count Sheet is designed to help healthcare providers track the administration and inventory of medications for residents. It ensures that accurate records are maintained, which is crucial for patient safety and compliance with regulations. By documenting the quantity of medication on hand, administered, and remaining, staff can prevent errors and ensure that residents receive their prescribed treatments on time.
What information is required on the Medication Count Sheet?
The Medication Count Sheet requires several key pieces of information. This includes the resident's name, the quantity of medication, the date the medication was started, the drug strength, and the staff signature. Additionally, it is important to record the date and time of administration, along with the quantities administered and remaining. This comprehensive data helps maintain an accurate medication log.
Who is responsible for filling out the Medication Count Sheet?
Staff members who are authorized to administer medications are responsible for completing the Medication Count Sheet. This typically includes nurses and certified nursing assistants. It is essential that the staff member who administers the medication also records the necessary details on the form to ensure accountability and accuracy in medication management.
How often should the Medication Count Sheet be updated?
The Medication Count Sheet should be updated each time medication is administered. This means that every dose given must be recorded immediately to reflect the current inventory accurately. Additionally, regular audits may be conducted to verify the information on the sheet against the actual medication supply, ensuring consistency and accuracy over time.
What should be done if there is a discrepancy in the medication count?
If a discrepancy is found in the medication count, it is crucial to report it immediately to a supervisor or the designated medication management personnel. Investigating the cause of the discrepancy should be a priority, as it could indicate a potential error in administration or record-keeping. Proper procedures should be followed to ensure that the issue is resolved and that patient safety is maintained.
Can the Medication Count Sheet be used for different types of medications?
Yes, the Medication Count Sheet can be used for various types of medications, including oral medications, injections, and topical treatments. It is a versatile tool that can accommodate different drug forms, as long as the necessary details are recorded. This adaptability makes it a valuable resource in various healthcare settings.
Is training required for staff to use the Medication Count Sheet?
Yes, staff should receive training on how to properly use the Medication Count Sheet. This training should cover the importance of accurate record-keeping, how to fill out the sheet correctly, and the protocols for reporting discrepancies. Ensuring that all staff members are knowledgeable about the process is essential for maintaining high standards of patient care.
What should be done with the Medication Count Sheet after it is filled out?
Once the Medication Count Sheet is filled out, it should be securely stored in accordance with the facility's policies on record retention. This ensures that the information remains accessible for audits and reviews while also protecting patient privacy. Regular reviews of these sheets can also help identify patterns or areas for improvement in medication management practices.
Inaccurate Quantity Entries: One common mistake occurs when individuals record the quantity of medication inaccurately. This can lead to confusion about how much medication is actually available. It’s essential to double-check the numbers before finalizing the entries.
Missing Staff Signatures: Failing to include the staff member's signature can create issues in accountability. Each entry should be verified and signed by the person administering the medication to ensure proper tracking and responsibility.
Omitting Dates: Dates play a crucial role in medication management. Omitting the date when the medication was administered or started can complicate records. Always ensure that each entry has a corresponding date to maintain clarity.
Incorrect Drug Strength Notation: Sometimes, the strength of the medication may be recorded incorrectly. This can have serious implications for patient care. It is important to carefully read the medication label and accurately transcribe the strength on the form.
Neglecting to Update Remaining Quantities: After administering medication, it is crucial to update the remaining quantity. Failing to do so can lead to discrepancies and may result in a shortage of medication for future doses.
The Medication Count Sheet is an essential tool used in healthcare settings to track the administration and inventory of medications. However, it is often accompanied by several other forms and documents that help ensure proper medication management and compliance with regulations. Below is a list of commonly used documents that complement the Medication Count Sheet.
Utilizing these forms and documents in conjunction with the Medication Count Sheet enhances the overall safety and effectiveness of medication management in healthcare settings. Each document plays a vital role in maintaining accurate records, ensuring compliance, and ultimately protecting patient health.
The Medication Administration Record (MAR) is a crucial document used in healthcare settings to track the administration of medications to patients. Similar to the Medication Count Sheet, the MAR includes essential details such as the patient’s name, medication name, dosage, and the times medications are to be given. Both documents serve the purpose of ensuring accurate medication management and accountability, providing a clear record of what has been administered and what remains. Staff signatures are often required on both forms to verify that medications have been given as prescribed.
The Inventory Control Sheet is another document that shares similarities with the Medication Count Sheet. This sheet is used to track the stock levels of medications and supplies within a healthcare facility. Like the Medication Count Sheet, it records quantities and dates, allowing for the monitoring of medication usage over time. Both documents help ensure that adequate supplies are maintained and that discrepancies in medication counts can be identified and addressed promptly.
The Prescription Log is also comparable to the Medication Count Sheet. This document records prescriptions written by healthcare providers, including patient details, medication names, dosages, and the date the prescription was issued. While the Medication Count Sheet focuses on tracking administered medications, the Prescription Log provides a broader view of medication management by capturing the initial prescribing process. Both documents are essential for maintaining an accurate medication history for patients.
The Controlled Substance Log is specifically designed for tracking controlled substances, which require more stringent oversight due to their potential for abuse. Similar to the Medication Count Sheet, this log includes details such as the drug name, quantity received, quantity administered, and remaining quantities. Both documents require staff signatures to confirm the accuracy of entries, ensuring compliance with regulatory standards and promoting accountability in medication handling.
The Patient Medication Profile is a document that provides a comprehensive overview of a patient’s medication regimen. It includes information about all medications prescribed, dosages, and any relevant allergies or interactions. While the Medication Count Sheet focuses primarily on tracking specific quantities and administration times, the Patient Medication Profile offers a more holistic view of a patient’s medication history. Both documents are vital for ensuring safe and effective medication management in a clinical setting.
When filling out the Medication Count Sheet form, attention to detail is crucial. Here are five important dos and don'ts to keep in mind:
By following these guidelines, you can help ensure that medication records are accurate and reliable. This is vital for the safety and well-being of all residents.
Understanding the Medication Count Sheet form is crucial for ensuring proper medication management. Here are ten common misconceptions about this form:
Addressing these misconceptions can enhance medication management practices and improve patient safety.
When using the Medication Count Sheet form, keep these key takeaways in mind: