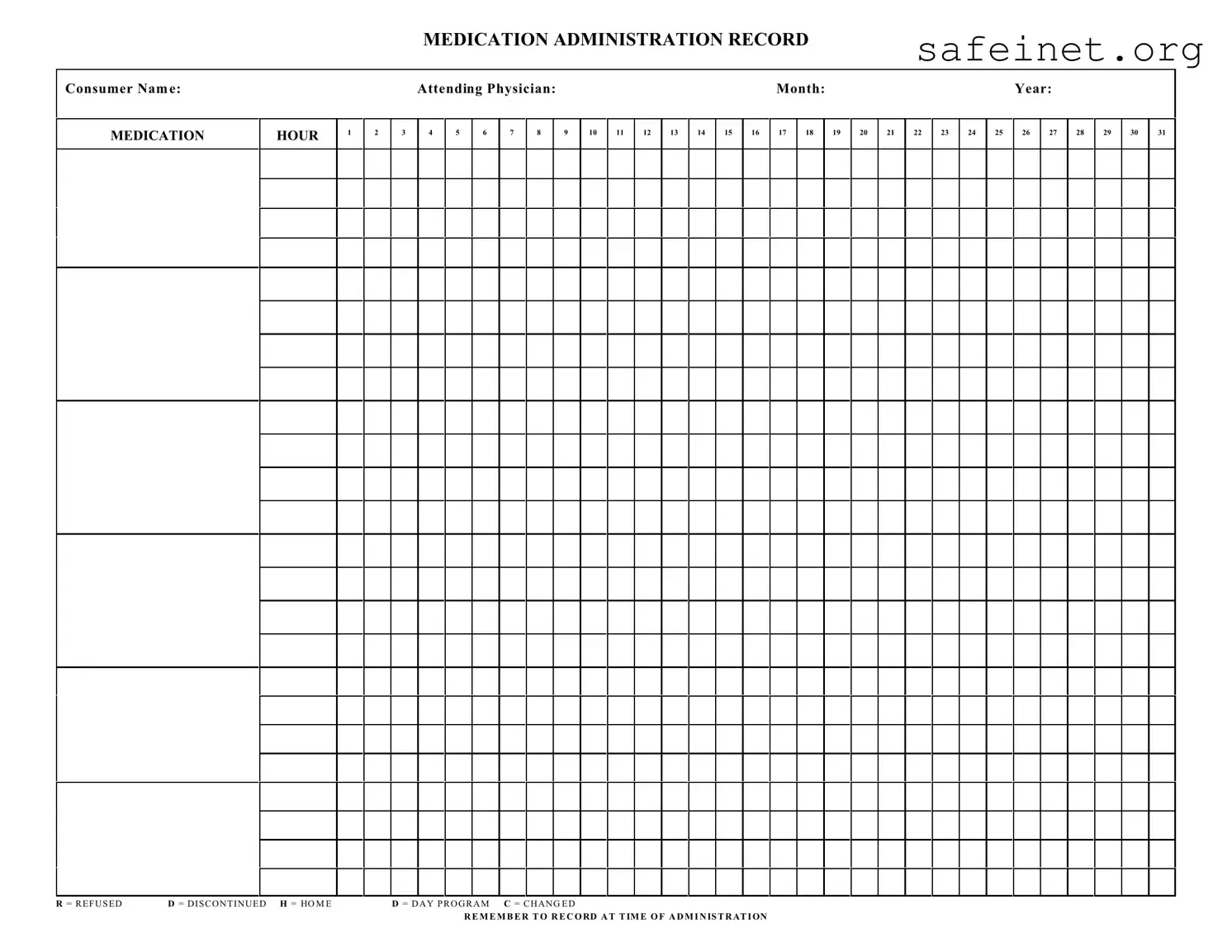
The Medication Administration Record Sheet, commonly referred to as MAR, serves as a critical tool in the healthcare setting for tracking medication administration to patients. This form is instrumental in documenting essential information such as the patient's name, the attending physician, and the month and year of medication records. It is organized in a way that denotes different hours throughout the day, allowing healthcare providers to indicate when medications are administered clearly. Additionally, several codes provide crucial information regarding the status of medication: 'R' for refused, 'D' for discontinued, 'H' for home, 'D' for day program, and 'C' for changed. Each entry plays an integral role in ensuring that the administration of medication is precise and timely, contributing to the overall safety and wellbeing of patients. Remember, recording medication administered at the correct time is vital not only for compliance but also for maintaining the integrity of patient care. The MAR form is more than just a piece of paper; it is an accountability tool that helps prevent errors and ensures that everyone involved in a patient's care is on the same page.
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
| Fact Name | Details |
|---|---|
| Purpose | The Medication Administration Record (MAR) records details about prescribed medications for consumers. |
| Patient Information | Consumer name must be clearly written to ensure accurate medication delivery. |
| Medical Oversight | The form requires the name of the attending physician for accountability. |
| Monthly Tracking | Spaces for each day of the month allow tracking of medication administration. |
| Administering Hours | Individual hour columns (1-24) indicate when medication was given or refused. |
| Status Notations | Standard codes (R, D, H, C) must be used to document medication status accurately. |
| Record-Keeping | It is crucial to record the administration time to maintain an accurate medication history. |
| State Requirements | Specific state laws govern the use of MAR forms, such as regulations from the Department of Health. |
| Training | Staff members must be trained on how to complete and interpret the MAR sheet correctly. |
| Confidentiality | All patient information on the MAR is protected under HIPAA, ensuring privacy is maintained. |
Filling out the Medication Administration Record Sheet is straightforward. The information collected is crucial for tracking medication administration for each consumer. Attention to detail is essential to ensure accuracy in documenting when and how medication is given.
What is a Medication Administration Record Sheet (MARS)?
A Medication Administration Record Sheet is a vital tool for tracking medication administered to a consumer. This form records various details, including the consumer's name, attending physician, and the specific month and year. It ensures that medication is given at the correct times while offering a clear record in case of inquiries or audits.
How do I use the Medication Administration Record Sheet?
To utilize the MARS, start by filling in the consumer's name, attending physician, and the date (month and year). When administering medication, note the hour in the corresponding box. If a medication is refused or discontinued, mark it as instructed: 'R' for refused and 'D' for discontinued. Remember to record all actions at the time of administration for accuracy.
What should I do if a medication is changed?
If a medication has been changed, indicate this on the MARS by marking 'C' in the box corresponding to the medication time. Ensure all staff members are aware of the change to avoid administration errors. It's crucial to follow up by updating any relevant documents regarding the consumer's medication regimen.
Why is it important to record medication administration accurately?
Accurate records are essential for multiple reasons. First, they help ensure consumer safety by preventing medication errors. Second, they provide essential documentation for healthcare providers to review the consumer's treatment history. In addition, proper recording can help comply with regulatory requirements to demonstrate accountability and transparency in medication management.
Incorrectly filling out the consumer's name. Ensuring the name is accurate and matches official records is crucial for proper medication management.
Failing to record the time of administration. It's essential to note the exact time when the medication was given to maintain proper documentation and avoid potential medication errors.
Neglecting to indicate refusals or discontinuations. If a consumer refuses medication or if a prescription is discontinued, noting this is important to reflect changes in treatment accurately.
Using incorrect abbreviations. Familiarity with the abbreviations used on the form is vital. Misunderstandings can lead to errors in administration.
Leaving sections blank. Completing every relevant section is necessary to ensure comprehensive and clear documentation.
Failing to update doses or changes in medication. Keeping the record current with any adjustments in medication or dosage is crucial for effective communication among healthcare providers.
Not signing or dating the record. After completing the form, it’s important to provide a signature and the date, confirming the action taken and establishing accountability.
The Medication Administration Record (MAR) Sheet is an essential tool for documenting the administration of medications to patients. Alongside this sheet, several other forms and documents can assist healthcare professionals in ensuring safe and effective medication management. Here is a list of commonly used documents that often accompany the MAR form.
These accompanying documents play a critical role in the overall process of medication administration. Together, they help create a comprehensive and safe system for managing patient care and improving health outcomes.
The Medication Administration Record (MAR) is similar to the Patient Medication Record (PMR), often found in clinical settings. Both documents serve to track medications prescribed to a patient. The PMR contains comprehensive details about a patient's medication history, including additional notes about allergies or previous reactions. Like the MAR, it helps ensure that healthcare providers convey correct information regarding medication management.
The nursing flow sheet is another document similar to the MAR. It is used for documenting the administration of medications as well as vital signs and observations made during a patient's care. Both sheets work together to provide an overview of a patient’s condition and response to treatment. The nursing flow sheet is often more extensive in scope, recording various clinical data alongside medication administration.
The Medication Reconciliation Form plays a key role in ensuring patient safety, much like the MAR. This form is utilized during transitions of care when a patient moves from one setting to another, helping to confirm the medications the patient is taking. Both documents prioritize accuracy in medication records, minimising the risk of errors when medications are prescribed or administered.
The Treatment Administration Record (TAR) resembles the MAR but focuses on non-medication treatments, such as oral hygiene or physiotherapy. Both records are essential for tracking the administration of care, ensuring patients receive comprehensive treatment as prescribed. They help caregivers maintain accurate logs and provide continuity of care.
Care Plans often have similarities with the MAR, particularly in that they outline goals and interventions for patient care, including medication management. While the MAR tracks actual medication administration, the Care Plan provides guidance on the intent and purpose of those medications. Together, both documents support coordinated patient care.
The Medication Dosage Record is another document similar to the MAR, specifically designed to track the dosages of medications administered at specific times. This record helps prevent overdosing and ensures compliance with the prescribed medication regimen. Both documents are crucial in documenting medication administration effectively.
The Daily Logbook shares features with the MAR, particularly in its role to track daily activities and medication administration. While the MAR focuses primarily on medications, the Daily Logbook captures all aspects of patient care for the day. Both documents provide a comprehensive picture of patient interactions and treatments.
The Prescription Order Form is also related to the MAR, as it indicates what medications have been prescribed for the patient. While the MAR reflects the actual administration of these medications, the Prescription Order Form captures the starting point—what physicians have recommended, including dosage and frequency. This ensures accuracy and adherence to the treatment plan.
When filling out the Medication Administration Record Sheet form, consider the following guidelines to ensure accuracy and compliance.
Understanding the Medication Administration Record Sheet (MAR) form is crucial for ensuring accurate medication management. However, several misconceptions can lead to confusion. Here are nine of those misunderstandings, clarified:
By dispelling these misconceptions, healthcare providers can better utilize the MAR, leading to improved patient care and safety.
When using the Medication Administration Record (MAR) Sheet form, it is important to keep a few crucial points in mind to ensure accurate record-keeping and patient safety. Here are some key takeaways:
By adhering to these points, you can maintain a clear and effective Medication Administration Record that promotes the well-being of individuals under your care.
Index Card Template Word - For side cards, you can change text direction for better visibility.
Sf33 - This fan chart can cultivate a deeper appreciation for family roots.