The Hospital Bill form serves as a crucial document for patients receiving care at healthcare facilities. It outlines the financial details associated with medical services rendered, including the total charges, payments made, and any adjustments to the account. Patients can find their personal information, such as name and address, prominently displayed at the top of the form. Additionally, the form includes essential payment instructions, allowing individuals to remit payment by check or credit card. For those who prefer online transactions, a website link is provided for convenience. The form also highlights the importance of updating personal and insurance information, ensuring that healthcare providers have the most accurate data on file. Furthermore, a summary of services, including charges for specific treatments like emergency room visits and pharmacy costs, is presented clearly. This transparency helps patients understand their financial responsibilities. Overall, the Hospital Bill form is designed to facilitate communication between patients and healthcare providers regarding billing and payment processes.
| Fact Name | Details |
|---|---|
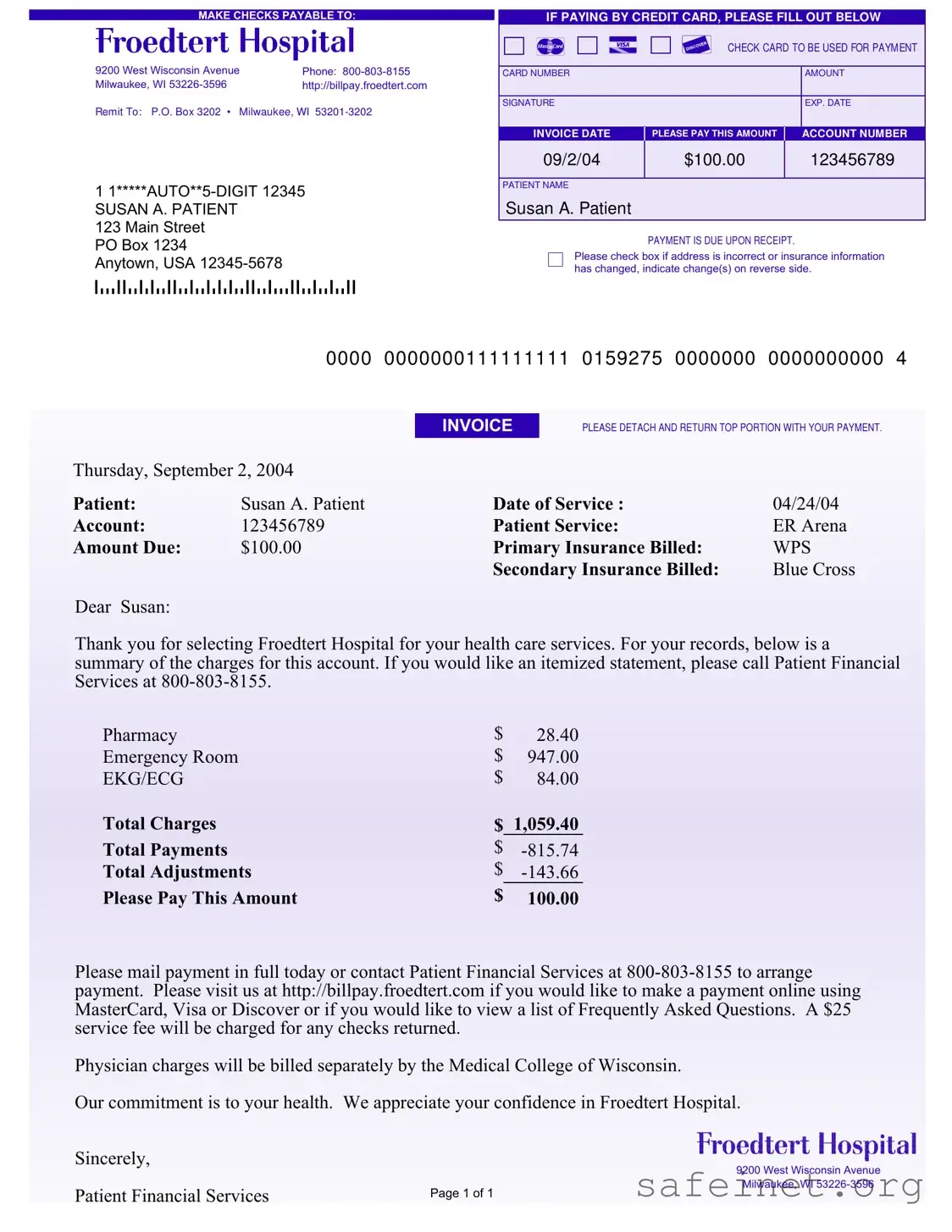
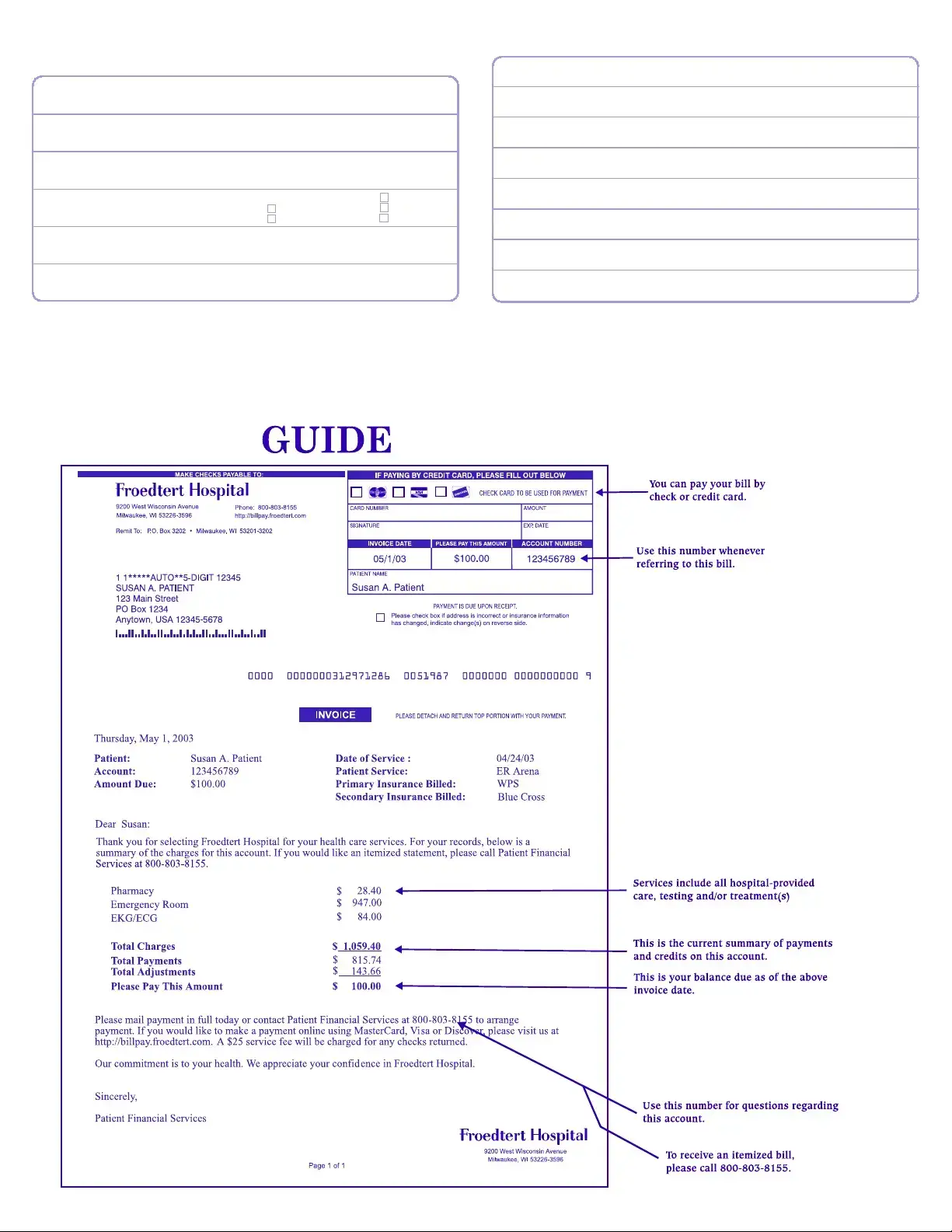
| Payment Instructions | Checks should be made payable to Froedtert Hospital. |
| Contact Information | Phone number for inquiries is 800-803-8155. |
| Remittance Address | Payments should be sent to P.O. Box 3202, Milwaukee, WI 53201-3202. |
| Invoice Date | The invoice date is September 2, 2004. |
| Payment Due | Payment is due upon receipt of the bill. |
| Insurance Information | Primary insurance billed is WPS; secondary insurance billed is Blue Cross. |
| Service Charges | Total charges amount to $1,059.40 with a balance due of $100.00. |
| Online Payment | Payments can be made online at http://billpay.froedtert.com. |
| Returned Checks | A $25 service fee applies for any returned checks. |
Completing the Hospital Bill form is a straightforward process that ensures your payment is processed efficiently. This form requires specific information about you, your insurance, and the payment method you prefer. Following the steps below will help you fill out the form accurately and promptly.
After completing the form, ensure that all information is accurate before mailing it to the address specified. This will help avoid any delays in processing your payment and keep your account in good standing.
What is the purpose of the Hospital Bill form?
The Hospital Bill form serves as a notification of the charges incurred during your visit to the hospital. It details the services provided, the total amount due, and payment instructions. This form is essential for ensuring that you understand your financial responsibilities regarding your healthcare services.
How do I make a payment for my hospital bill?
You can make a payment by mailing a check to the address provided on the form or by visiting the online payment portal at http://billpay.froedtert.com. If you prefer to pay by credit card, fill out the designated section on the form, including your card number, expiration date, and the amount you wish to pay.
What should I do if my address or insurance information has changed?
If your address or insurance information has changed since your last statement, please check the box indicated on the form. You should also provide the updated information on the reverse side of the form to ensure your records are accurate and up to date.
What happens if my payment is returned?
If a check is returned for any reason, a $25 service fee will be charged. It is important to ensure that you have sufficient funds in your account to cover the payment to avoid this fee.
Can I request an itemized statement of my charges?
Yes, if you would like a detailed breakdown of your charges, you can call Patient Financial Services at 800-803-8155. They will assist you in obtaining an itemized statement for your records.
What should I do if I have questions about my bill?
If you have any questions or concerns regarding your bill, you can reach out to Patient Financial Services at the provided phone number. They are available to help clarify any charges or payment arrangements you may need assistance with.
When is payment due for my hospital bill?
Payment is due upon receipt of the bill. It is advisable to address the payment as soon as possible to avoid any potential late fees or complications with your account.
What if I have both primary and secondary insurance?
The form indicates that both your primary and secondary insurance will be billed. Make sure to provide accurate information about both insurance providers to ensure proper billing. If there are any discrepancies or issues with coverage, contact your insurance companies directly.
What services are included in the total charges?
The total charges listed on the form include various services such as pharmacy, emergency room visits, and any tests performed, like EKG/ECG. The breakdown of these charges is provided for your reference, allowing you to see where the costs are allocated.
Who will bill for physician charges?
Physician charges will be billed separately by the Medical College of Wisconsin. You may receive a different bill for these services, so be prepared to manage multiple bills related to your care.
Ignoring the Instructions: Many people overlook the specific instructions provided on the hospital bill form. This can lead to incomplete submissions or errors in processing payments.
Incorrect Payment Amount: Double-check the amount due. Some individuals mistakenly pay more or less than what is indicated, which can complicate their account status.
Missing Signature: Forgetting to sign the form is a common mistake. Without a signature, the payment may not be processed, leading to delays.
Using an Incorrect Address: If your address has changed, it’s crucial to update it on the form. An outdated address can cause important documents to be sent to the wrong location.
Not Providing Insurance Information: Failing to fill out insurance details can lead to unexpected out-of-pocket costs. Make sure to include all relevant insurance information.
Overlooking Expiration Dates: When paying by credit card, ensure that the expiration date is current. An expired card will result in payment failure.
Forgetting to Detach the Payment Portion: Some people forget to detach the top portion of the bill. This can cause confusion and delays in processing your payment.
Not Keeping a Copy: Always retain a copy of the completed form for your records. This can be helpful if any issues arise later.
Neglecting to Contact Financial Services: If there are any questions or concerns, it’s important to reach out to Patient Financial Services for clarification before submitting the form.
The Hospital Bill form is a crucial document for patients to manage their medical expenses. In addition to this form, several other documents are often utilized to facilitate the billing and payment process. Below is a list of these related documents, each with a brief description.
Understanding these documents can help patients navigate their healthcare expenses more effectively. Each form serves a specific purpose in ensuring that billing processes are transparent and manageable.
The Hospital Bill form shares similarities with an Invoice form. Both documents detail charges incurred for services rendered. An invoice typically includes a breakdown of costs, payment due dates, and instructions for payment. Like the Hospital Bill, it specifies the total amount due and may provide a summary of services, allowing the recipient to understand what they are being charged for. Invoices often serve as a formal request for payment, similar to how a hospital bill requests payment for medical services.
Another document comparable to the Hospital Bill is the Explanation of Benefits (EOB) statement. An EOB is issued by an insurance company after a claim is processed. It outlines the services billed, the amount covered by insurance, and the remaining balance owed by the patient. Both documents aim to inform the patient about their financial responsibility, detailing what services were provided and how much the insurance has paid versus what the patient must pay. The EOB helps clarify the billing process, much like the Hospital Bill does.
The Patient Statement is also similar to the Hospital Bill. This document provides a summary of a patient's account, including outstanding balances, payments made, and any adjustments. It serves to keep patients informed about their financial obligations. Like the Hospital Bill, a Patient Statement may include specific details about services received and the total amount due. Both documents are essential for patients to track their healthcare expenses and manage their payments effectively.
A Medical Receipt is another document that bears resemblance to the Hospital Bill. After payment is made, a medical receipt confirms that the payment has been received for specific services. It includes details such as the date of service, amount paid, and a description of the services rendered. Similar to the Hospital Bill, it provides a record of transactions and serves as proof of payment, which is vital for patients who may need to submit claims to insurance companies.
Lastly, the Payment Plan Agreement can be compared to the Hospital Bill. This document outlines the terms of a payment arrangement between the patient and the healthcare provider. It specifies the total amount owed, the payment schedule, and any interest or fees associated with the plan. Like the Hospital Bill, it emphasizes the financial responsibility of the patient and provides clarity on how payments will be managed over time. Both documents are crucial for ensuring that patients understand their obligations and can make informed financial decisions regarding their healthcare costs.
When filling out the Hospital Bill form, it’s important to be thorough and accurate. Here’s a helpful list of what you should and shouldn’t do:
By following these tips, you can help ensure that your bill is processed smoothly and efficiently. Remember, accuracy is key!
Misconceptions about the Hospital Bill form can lead to confusion and frustration. Below are ten common misconceptions, along with clarifications for each.
Understanding these points can help patients navigate their hospital billing more effectively.
Here are some important points to remember when filling out and using the Hospital Bill form: