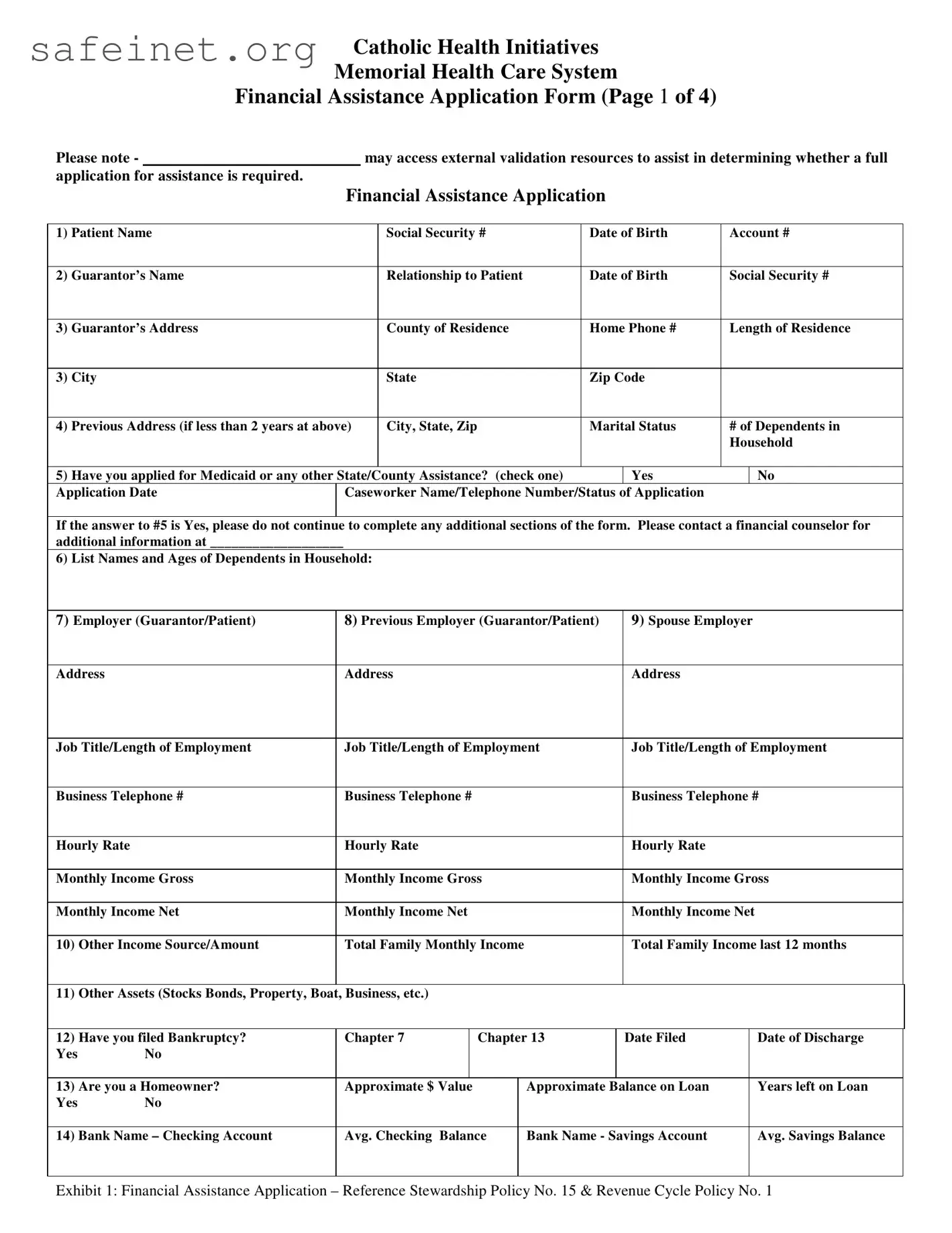
The Financial Assistance Application form provided by the Catholic Health Initiatives Memorial Health Care System serves as a vital tool for patients seeking financial relief in meeting their medical expenses. This comprehensive document requires essential personal information, such as the patient’s name, social security number, and date of birth, as well as details about their guarantor, including relationship, employment, and income information. Important sections address dependents and prior medical assistance applications, guiding users on what to do if they have already sought other forms of aid, such as Medicaid. Furthermore, applicants must articulate their financial status, detailing sources of income, assets, and monthly expenses such as housing, food, and medical costs. For a complete assessment, the form emphasizes the need for income verification and might prompt applicants to include additional documentation like bank statements and tax returns. Once completed, the signed application must be submitted to the financial assistance department to initiate the evaluation process, ultimately aiming to alleviate the burdens of healthcare costs for those in need.
Catholic Health Initiatives
Memorial Health Care System
Financial Assistance Application Form (Page 1 of 4)
Please note - |
|
|
may access external validation resources to assist in determining whether a full |
||||||
application for assistance is required. |
|
|
|
|
|
|
|
||
|
|
|
Financial Assistance Application |
|
|
||||
|
|
|
|
|
|
|
|
|
|
1) |
Patient Name |
|
|
Social Security # |
Date of Birth |
Account # |
|||
|
|
|
|
|
|
|
|
|
|
2) |
Guarantor’s Name |
|
|
Relationship to Patient |
Date of Birth |
Social Security # |
|||
|
|
|
|
|
|
|
|
|
|
3) |
Guarantor’s Address |
|
|
County of Residence |
Home Phone # |
Length of Residence |
|||
|
|
|
|
|
|
|
|
|
|
3) |
City |
|
|
State |
Zip Code |
|
|
||
|
|
|
|
|
|
|
|
|
|
4) |
Previous Address (if less than 2 years at above) |
|
City, State, Zip |
Marital Status |
# of Dependents in |
||||
|
|
|
|
|
|
|
|
Household |
|
|
|
|
|
|
|
|
|
||
5) |
Have you applied for Medicaid or any other State/County Assistance? (check one) |
|
Yes |
|
No |
||||
Application Date |
Caseworker Name/Telephone Number/Status of Application |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
If the answer to #5 is Yes, please do not continue to complete any additional sections of the form. Please contact a financial counselor for additional information at ___________________
6) List Names and Ages of Dependents in Household:
7) Employer (Guarantor/Patient) |
8) Previous Employer (Guarantor/Patient) |
9) Spouse Employer |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
Address |
Address |
|
|
|
|
Address |
|
|||
|
|
|
|
|
|
|
||||
Job Title/Length of Employment |
Job Title/Length of Employment |
Job Title/Length of Employment |
||||||||
|
|
|
|
|
|
|
|
|
||
Business Telephone # |
Business Telephone # |
|
|
|
|
Business Telephone # |
||||
|
|
|
|
|
|
|
|
|
|
|
Hourly Rate |
Hourly Rate |
|
|
|
|
Hourly Rate |
|
|||
|
|
|
|
|
|
|
|
|||
Monthly Income Gross |
Monthly Income Gross |
|
|
Monthly Income Gross |
||||||
|
|
|
|
|
|
|
|
|
|
|
Monthly Income Net |
Monthly Income Net |
|
|
|
|
Monthly Income Net |
|
|||
|
|
|
|
|
|
|
|
|
||
10) |
Other Income Source/Amount |
Total Family Monthly Income |
|
|
Total Family Income last 12 months |
|||||
|
|
|
|
|
|
|
|
|
|
|
11) |
Other Assets (Stocks Bonds, Property, Boat, Business, etc.) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
12) |
Have you filed Bankruptcy? |
Chapter 7 |
|
Chapter 13 |
|
Date Filed |
|
Date of Discharge |
||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
13) Are you a Homeowner? |
Approximate $ Value |
|
|
Approximate Balance on Loan |
|
Years left on Loan |
||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
14) Bank Name – Checking Account |
Avg. Checking Balance |
|
Bank Name - Savings Account |
|
Avg. Savings Balance |
|||||
|
|
|
|
|
|
|
|
|
|
|
Exhibit 1: Financial Assistance Application – Reference Stewardship Policy No. 15 & Revenue Cycle Policy No. 1
Catholic Health Initiatives
Memorial Health Care System
Financial Assistance Application Form (Page 2 of 4)
15) AUTOMOBILE(S) |
|
|
|
|
|
|
|
|
|
1. Make: |
|
Model: |
|
Year: |
Pymt Amount: |
Balance Due: |
|||
|
|
|
|
|
|
|
|
|
|
2. Make: |
|
Model: |
|
Year: |
Pymt Amount: |
Balance Due: |
|||
|
|
|
|
|
|
|
|
|
|
3. Make: |
|
Model: |
|
Year: |
Pymt Amount: |
Balance Due: |
|||
|
|
|
|
|
|
|
|
|
|
4. Make: |
|
Model: |
|
Year: |
Pymt Amount: |
Balance Due: |
|||
|
|
|
|
|
|
|
|
|
|
Monthly Expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Description |
|
Monthly Payment |
Payment To |
|
Balance Due |
|
Limit |
||
Rent/Mortgage |
|
$ |
|
|
|
|
$ |
|
$ |
Charge Cards |
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
Bank Loans |
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
|
|
$ |
|
|
|
|
$ |
|
$ |
School Loans |
|
$ |
|
|
|
|
$ |
|
$ |
List Other Expenses Below:
|
Monthly Payment |
|
Monthly Payment |
|
Monthly Payment |
|
FOOD |
$ |
|
MEDICATION |
$ |
AUTO INS |
$ |
UTILITIES |
$ |
|
LIFE INSURANCE |
$ |
OTHER |
$ |
GAS (CAR) |
$ |
|
MEDICAL BILLS |
$ |
OTHER |
$ |
TOTAL MONTHLY EXPENSE |
$ |
|
|
|
|
|
Note: Attach additional sheet if necessary. Important: income verification must be attached – W2, Pay Stub, Tax Return with schedules, etc.
PLEASE READ THE FOLLOWING BEFORE SIGNING AND DATING THE APPLICATION
Please be advised that your signature indicates you have agreed to attach all income verification. In addition to the items requested by this application, you may attach bank statements, copies of social security checks (or letters). If there is no income, please verify how expenses are being met. It is important to explain a lack of income completely so that full consideration of your application can be made. If the guarantor/patient or the spouse is
CERTIFICATION
1.I, the undersigned, certify that the completed information in this document is true and accurate to the best of my knowledge.
2.I will apply for any and all assistance that may be available to help pay this bill.
3.I understand the information submitted is subject to verification; therefore, I grant permission and authorize any bank, insurance co., real estate co., financial institution and credit grantors of any kind to disclose to any authorized agent of
________________ information as to my past and present accounts, policies, experiences and all pertinent information related thereto. I authorize _____________________ to perform a credit check for both guarantor/patient and spouse.
Signature (Guarantor/Patient)
Date
Signature (Spouse)
Date
Please complete and mail your Financial Assistance Application to: Attn: Business Office - Financial Assistance Request, Memorial Health Care System, 2525 de Sales Avenue, Chattanooga, TN 37404
Exhibit 1: Financial Assistance Application – Reference Stewardship Policy No. 15 & Revenue Cycle Policy No. 1
Catholic Health Initiatives
Memorial Health Care System
Financial Assistance Application Form (Page 3 of 4)
DIRECTIONS FOR COMPLETING FINANCIAL ASSISTANCE APPLICATION
1: Complete the patient name, patient’s social security number, patient’s date of birth, and the hospital account number(s) if known.
2: Complete the guarantor name, relationship to patient, guarantor’s date of birth, and guarantor’s social security number. If the guarantor is the same as the patient, note “Same” in this field.
3: Complete the guarantor’s address, home telephone number and length of residence at this address.
4: Complete the guarantor’s previous address (if current residence is less than two years), guarantor’s marital status, and number of dependents living in household. If there are no dependents, please mark
5: Complete the questions regarding Medicaid and other State/County assistance. Please advise if you have applied for assistance (and on what date). Provide the assigned Caseworker’s name, telephone number and the status of the application. You may attach a separate sheet if needed. If your response is “Yes”, please do not proceed to complete any additional sections of the form. Please contact a financial counselor for additional information. If this section does not apply to you, please indicate this by marking it with N/A.
6: List the names and ages of dependents.
7: Complete the employer information for the guarantor or patient, depending upon who has responsibility for the balance. Please complete the name of the employer, the employer’s address, the guarantor/patient’s job title and length of employment. Please also include the guarantor/patient’s business telephone number, hourly (or salary) rate, and the monthly income (both gross and net). If there is no employment, please note how expenses are being met.
8: Complete the previous employer information for the guarantor/patient. This includes the employer’s name and address, the guarantor/patient’s job title and length of employment, business telephone number, hourly rate, and monthly income (both gross and net). If there is no prior employment, mark “N/A”.
9: Complete the income information for the guarantor/patient’s spouse. Include the name of the employer, the employer’s address, job title/length of employment, business telephone number, hourly rate, and monthly income (both gross and net). If the spouse is unemployed, or there is no spouse, mark “N/A”.
10: Complete the other income source/amount. This is for child support, social security, bonus amounts from employers, etc. This also includes rental income, alimony, pension income, welfare and VA benefits. Complete the total family income (add the guarantor/patient net income), then complete the total family income from the last 12 months. If there has been no income, please note how expenses are being met.
11:Please complete the section listing other assets you may have. This includes stocks, bonds, property, boats and businesses you may own. Use additional paper if needed to give complete details. If there are no additional assets, please mark “N/A”.
12: Please indicate if you have ever filed bankruptcy. If you have not filed bankruptcy, please mark “No”. Please verify that all questions have been completed. Attach additional paper if needed for any explanations.
13: Please complete the homeowner information. If you are a homeowner, please note the approximate dollar value, the approximate balance on the loan, and the number of years left on the loan. If you are not a homeowner, please mark “No”.
14: Please complete the banking information as requested and list the bank name. Complete the checking account number and provide the average checking account balance. Please do the same for the savings account field. If there is no savings account, please place “N/A” in the savings field.
15: For automobile information, please list the make, model and year of your vehicle. Please list the monthly payment amount and the current balance. Attach additional documentation for more than four autos.
Exhibit 1: Financial Assistance Application – Reference Stewardship Policy No. 15 & Revenue Cycle Policy No. 1
Catholic Health Initiatives
Memorial Health Care System
Financial Assistance Application Form (Page 4 of 4)
HOW TO COMPLETE THE MONTHLY EXPENSE SECTION (copies of monthly bills/statements may be requested):
RENT/MORTGAGE: Please verify the amount you are paying in rent or by mortgage. Indicate to whom the payment is made, the account number and the current balance due. If you do not pay rent or mortgage, please note why you have no payment or if you live with relatives or others. Use additional paper if needed.
CHARGE CARDS: Please indicate any charge card payments you are currently making. Please indicate the monthly payment amount, to whom the payment is made, the account number and the current balance due. Please indicate the credit limit for each card. Use additional paper if you needed to complete this field. If you have no charge cards please note “N/A”.
BANK LOANS: Please indicate any bank loans you may be paying. Indicate the monthly payment amount, to whom the payment is made, the account number and the current balance due. Use additional paper if needed to completely explain this field. If you have no bank loans, please mark “N/A”.
SCHOOL LOANS: Please list any educational loans you may be paying. This can include, but not be limited to, college loans, private school loans (or tuition),
LIST OTHER MONTHLY EXPENSES:
FOOD: Please list the amount paid for food on a monthly basis.
UTILITIES: Please list the amount paid on a monthly basis for electricity, gas, water, trash and any other utility you may pay. Please add these and place the total (for all of them) in the utilities section. If there are no monthly utilities paid, please mark “N/A” in this section and explain. Use a separate sheet of paper if needed.
GAS (CAR): Please list the amount paid on a monthly basis for transportation needs related to your vehicle. If there is no payment made on a monthly basis for gas, please mark the field “N/A”.
MEDICATION: Please add the amounts you pay on a monthly basis for medication needs. If there are several prescriptions or medications you take, please add them together and place the total amount in this section. If there are no monthly medication payments, please place “NA” in this section.
LIFE INSURANCE: If you have a life insurance policy, please indicate the monthly amount you pay. If there is no payment, please place “N/A” in this section.
MEDICAL BILLS: Please add any medical bills you may be paying on a monthly basis. This may include, but not be limited to, physician bills, insurance
AUTO INSURANCE: Please place the total amount you pay on a monthly basis for auto insurance. If you pay on a quarterly basis, please divide the quarterly payment by three and place the amount in this section. If you pay every six months, please divide the total amount you pay by six and place the amount in this section. If there is no monthly payment being made, please mark N/A in this section.
OTHER: This includes any monthly payments you currently are making that are not listed in the previous sections. Please provide details of what you are paying, to whom, and the balances due. Please use a separate sheet of paper if needed. If this section does not apply to you, mark “N/A”.
TOTAL MONTHLY EXPENSES: Please estimate your monthly expenses and place this amount in this section.
Exhibit 1: Financial Assistance Application – Reference Stewardship Policy No. 15 & Revenue Cycle Policy No. 1
| Fact Name | Description |
|---|---|
| Application Purpose | This form is used to apply for financial assistance for medical expenses through Memorial Health Care System. |
| Eligibility Verification | Applicants must attach income verification documents, such as W2s, pay stubs, or tax returns. |
| Dependents Information | Applicants need to list the names and ages of all dependents living in the household. |
| Bankruptcy Disclosure | Applicants must disclose if they have filed for bankruptcy, including the chapter and dates. |
| Contact Information | Applicants can reach out to a financial counselor if they have questions or need assistance completing the form. |
| State-Specific Law | This application is governed by the laws of Tennessee regarding financial assistance programs. |
Once you have your Financial Assistance Application form in front of you, follow these steps to complete it accurately. Ensure you have all necessary documents, such as income verification, ready for submission. After filling out the form, mail it to the appropriate address provided in the instructions.
1. What is the purpose of the Financial Assistance Application form?
This form is designed to help individuals and families request financial assistance for medical bills. It collects key information about the patient's financial situation to determine eligibility for assistance programs. By filling out this application, you can help ensure that you receive the financial support you may need.
2. Who should fill out the application?
The application should be filled out by the patient or the guarantor—this is the person responsible for the medical bills. If the guarantor is the same as the patient, simply note “Same” in the relevant section.
3. What information is required on the application?
The form requires personal details such as names, social security numbers, and addresses, as well as financial information including income, expenses, assets, and debts. Additionally, you will need to provide details about dependents and any previous assistance applications.
4. What should I do if I have already applied for Medicaid or state assistance?
If you have applied for Medicaid or other state assistance, you should stop filling out the application and contact a financial counselor. They can guide you on the next steps and help you navigate the assistance process.
5. What types of income need to be reported?
You should report all sources of income, including wages, child support, social security benefits, rental income, and any other financial support you receive. Be thorough to ensure an accurate picture of your financial situation.
6. Do I need to provide documentation with my application?
Yes, it’s important to include documentation like W-2 forms, pay stubs, or tax returns to verify income. If you have no income, you should explain how your monthly expenses are covered. Incomplete applications may be returned, so be sure to attach all necessary documents.
7. How long will it take to process my application?
The processing time can vary based on the details of your application and the volume of requests being handled. It is best to ask your financial counselor for an estimated timeline once you submit your application.
8. What happens if my financial situation changes after I submit the application?
If your financial situation changes after you submit your application, it’s important to inform the financial counselor as soon as possible. Changes such as job loss or unexpected expenses can impact your eligibility and the type of assistance you may qualify for.
9. Where should I send my completed application?
Your completed application should be mailed to the Memorial Health Care System's Business Office. The address is 2525 de Sales Avenue, Chattanooga, TN 37404. Double-check that you have included all necessary documentation before mailing to avoid delays.
Omitting Required Identification: Some applicants forget to include their full names, Social Security numbers, and dates of birth. Accurate personal identification is critical for processing the application.
Failing to Specify Guarantor Information: If the guarantor is not the same as the patient, it’s common to miss this critical detail. This can lead to processing delays.
Neglecting Previous Addresses: Leaving out previous addresses can cause issues in background checks and eligibility assessments. Make sure to note any address changes within the last two years.
Inaccurate Income Reporting: Providing incorrect figures for monthly income or failing to list additional income sources can lead to miscalculations. Always double-check these figures.
Ignoring Medicaid Section: If you have applied for Medicaid, do not fill out the rest of the form. Skipping or misunderstanding this part could nullify your application.
Submitting Incomplete Documentation: Income verification documents must accompany the application. Forgetting to include W2s or recent pay stubs can result in delays.
Not Detailing Dependents: Accurately listing dependents, including ages, is crucial. Misreporting this information can affect financial eligibility.
Overlooking Assets Section: Failing to disclose assets like property, stocks, or savings can be seen as withholding information, impacting the application outcome.
Bypassing Expense Details: It’s important to list all monthly expenses. Omitting even minor expenses can skew the monthly budget analysis and affect assistance levels.
Missing Signatures and Dates: Signatures of both the guarantor and spouse, along with the date, should be affixed at the end. Applications submitted without these can be deemed incomplete.
The Financial Assistance Application Form is often accompanied by several additional forms and documents that help verify financial circumstances. Below is a list of these documents commonly required for the application process.
Submitting these documents along with the Financial Assistance Application Form can help facilitate the review process. Comprehensive documentation allows for a clearer understanding of financial needs and supporting background information.
The Medicaid Application is closely related to the Financial Assistance Application form. It serves a similar purpose by collecting essential information to determine eligibility for financial aid regarding health care expenses. Both forms ask for personal details such as names, social security numbers, and income information. A critical distinction is that the Medicaid Application specifically focuses on state-funded assistance programs, while the Financial Assistance Application can encompass various types of financial aid from different sources.
The Employment Verification Request is another document akin to the Financial Assistance Application. Like the latter, it gathers information about employment history and income. Both forms require details regarding the employer's name, address, and the employee's job title. However, the Employment Verification Request primarily seeks to confirm someone's current employment status, while the Financial Assistance Application also collects information about dependents, assets, and specific financial hardships.
The IRS Form 1040, used for personal income tax returns, shares similarities with the Financial Assistance Application as both require detailed financial information. Each collects income sources and amounts, enabling parties to analyze a person's financial status accurately. While the IRS Form 1040 is used for tax purposes, it serves as a resource for proving income in the Financial Assistance Application. Applicants often use tax forms to verify income levels and fulfill documentation requirements.
The Loan Application Form also bears resemblance to the Financial Assistance Application. Both documents inquire about the applicant's financial health and ability to repay a loan or obtain financial assistance. They require detailed information regarding income, assets, and monthly expenses. A key difference is that the Loan Application is focused on seeking funds for a specific purpose, such as purchasing a home, while the Financial Assistance Application aims to assess eligibility for support with existing medical expenses.
Finally, the Housing Assistance Application aligns with the Financial Assistance Application regarding its intent to evaluate the applicant's financial circumstances. Each form captures details about the individual's income and expenses, with the Housing Assistance Application focusing primarily on housing costs. Both aim to determine eligibility for assistance programs, though they differ in application scope, with the Housing Assistance Application focusing strictly on housing-related expenses.
Things You Should Do:
Things You Shouldn't Do:
Here are five common misconceptions about the Financial Assistance Application form:
The Financial Assistance Application is a vital document for those seeking financial help with medical expenses. Below are key takeaways to consider when filling out and using this form:
Filling out the form completely and accurately increases the chance of receiving the assistance needed. Be thorough and diligent to avoid delays in the application process.