The Express Scripts Fax form plays a crucial role in the process of submitting prescription drug claims for reimbursement. This form is designed for cardholders to provide important personal information, including their name, contact details, and insurance information. It allows users to specify the relationships of patients to the cardholder, making it clear who the claim is for, whether it be themselves, a spouse, child, or domestic partner. Additionally, the form requires essential details about prescriptions such as the pharmacy that filled them, the prescribing physician, and relevant identification numbers. Each claim submission needs to include necessary documentation, ensuring that the information provided is complete to prevent delays in processing. There are also sections to note claims for diabetic supplies and allergy serum, adding specificity to the type of medications being claimed. With the right information, the Express Scripts Fax form streamlines the claims process, ensuring that eligible individuals receive the benefits they are entitled to. Any omissions or inaccuracies can lead to returned claims, which underscores the importance of carefully reviewing the instructions provided on the form.
сЛГЛ E ?Л.?« СДІЛЛ S |
PRESCRIPTION DRUG CLAIM FORM |
||
Cardholder’s Name (last, first, Ml) |
Date Of Birth |
Gender |
Cardholder ID Number |
|
|
M |
F |
Check if new address |
|
|
|
Address Street |
|
|
|
Citv/State |
Zip Code |
|
Davtime Telephone ( ) |
Employer |
Insurance Carrier |
|
Group Number |
PLEASE SIGN AND DATE HERE: I certify that all information provided is correct and that the prescription(s) submitted are for me or members of my family who are eligible. The patient(s) listed below has (have) received the medication, and I authorize release of all information contained on this claim to Express Scripts, Inc. and my Plan Sponsor.
Cardholder’s Signature |
Date |
Patient Information (please list information For each patient submitting claims)
1 |
Patient’s Name |
Relationship to |
Gender Date of Birth |
How many |
|
|
Cardholder?(circle) |
(circle) |
prescriptions |
||
|
|
Self, Spouse, Child, Domestic Partner |
M |
F |
attached? |
Pharmacy Name and Address: |
|
Physician Name (name of prescribing Doctor) and DEA#: |
|||
2 |
Patient’s Name |
Relationship to |
|
Cardholder?(circle) |
|
|
|
Self, Spouse, Child, Domestic Partner |
Pharmacy Name and Address: |
|
|
3 |
Patient's Name |
Relationship to |
|
Cardholder?(circle) |
|
Self, Spouse, Child, Domestic Partner
Pharmacy Name and Address
Gender Date of Birth |
How many |
|
(circle) |
prescriptions |
|
M |
F |
attached? |
Physician Name (name of prescribing Doctor) and DEA#:
Gender Date of Birth |
How many |
|
(circle) |
prescriptions |
|
M |
F |
attached? |
Physician Name (name of prescribing Doctor) and DEA#:
Is claim for Diabetic Supply? □yesdno. If Yes, Patient's name |
|
|
|
|
Type of supply (lancets, syringe, etc.) |
Quantity |
Days Supply |
||
Does the patient reside in an assisted living facility? |
yes EJno |
Is this claim for allergy serum? |
yes dno |
|
Does the patient have primary prescription drug coverage through another insurance carrier? dyes dno
Prescription Information
■» IMPORTANT^- All prescription claims must have prescriptions receipts/labels which include:
• Pharmacy Name/Address • Date Filled • Drug Name, Strength and NDC • Rx Number • Quantity • Days Supply • Price «Patient’s Name
Claims received missing any of the above information may be returned or payment may be denied or delayed
ИPlease tape receipts to separate piece of paper
(3 Patient history print outs from the pharmacy are also acceptable but MUST be signed by the Pharmacist.
ECASH REGISTER RECEIPTS ARE NOT ACCEPTABLE FOR ANY PRESCRIPTIONS.
(With the exception of diabetic supplies)
REASON FOR CLAIM SUBMISSION OR SPECIAL NOTES: |
L esi Use only |
PLEASE READ THE FOLLOWING INSTRUCTIONS CAREFULLY AND COMPLETE
FORM ON REVERSE SIDE.
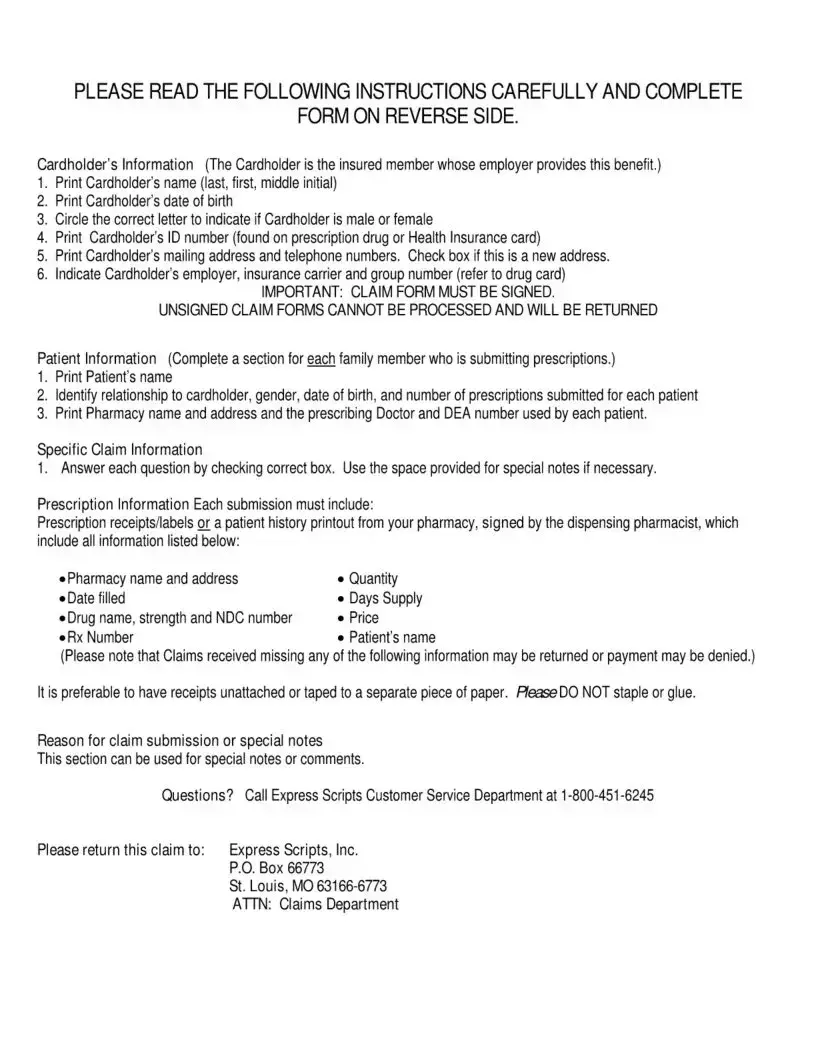
Cardholder’s Information (The Cardholder is the insured member whose employer provides this benefit.)
1.Print Cardholder's name (last, first, middle initial)
2.Print Cardholder’s date of birth
3.Circle the correct letter to indicate if Cardholder is male or female
4.Print Cardholder’s ID number (found on prescription drug or Health Insurance card)
5.Print Cardholder’s mailing address and telephone numbers. Check box if this is a new address.
6.Indicate Cardholder's employer, insurance carrier and group number (refer to drug card)
IMPORTANT: CLAIM FORM MUST BE SIGNED.
UNSIGNED CLAIM FORMS CANNOT BE PROCESSED AND WILL BE RETURNED
Patient Information (Complete a section for each family member who is submitting prescriptions.)
1.Print Patient’s name
2.Identify relationship to cardholder, gender, date of birth, and number of prescriptions submitted for each patient
3.Print Pharmacy name and address and the prescribing Doctor and DEA number used by each patient.
Specific Claim Information
1.Answer each question by checking correct box. Use the space provided for special notes if necessary.
Prescription Information Each submission must include:
Prescription receipts/labels or a patient history printout from your pharmacy, signed by the dispensing pharmacist, which include all information listed below:
• Pharmacy name and address |
• Quantity |
• Date filled |
«Days Supply |
• Drug name, strength and NDC number |
• Price |
• Rx Number |
• Patient's name |
(Please note that Claims received missing any of the following information may be returned or payment may be denied.)
It is preferable to have receipts unattached or taped to a separate piece of paper. HeaseDO NOT staple or glue.
Reason for claim submission or special notes
This section can be used for special notes or comments.
Questions? Call Express Scripts Customer Service Department at 1
Please return this claim to: |
Express Scripts, Inc. |
|
P.O. Box 66773 |
|
St. Louis, MO |
|
ATTN: Claims Department |
| Fact Name | Description |
|---|---|
| Form Purpose | This form is designed for submitting prescription drug claims to Express Scripts. |
| Cardholder Information | Cardholder details such as name, ID number, and employer are required for claim processing. |
| Signature Requirement | Claims must be signed by the cardholder; unsigned forms will be returned and not processed. |
| Patient Details | A separate section is required for each patient, including their relationship to the cardholder. |
| Prescription Attachments | All claims must include prescription receipts or labels with essential information listed. |
| Eligibility Confirmation | The cardholder certifies that the information is accurate and that the prescriptions are for eligible individuals. |
| Claim Submission Address | Claims must be sent to Express Scripts, P.O. Box 66773, St. Louis, MO 63166-6773. |
| Special Notes Section | The form includes a section for any special notes or additional comments regarding the claim. |
| Compliance with Regulations | The form must comply with relevant state laws and insurance regulations governing prescription claims. |
Filling out the Express Scripts Fax form requires careful attention to detail. Each section must be completed accurately to ensure the claim is processed smoothly. Follow these steps to fill out the form correctly.
For the Patient Information section, repeat the following steps for each family member submitting claims:
Complete the Specific Claim Information section by providing answers to each question and using the special notes space, if necessary. In the Prescription Information section, compile all receipts or patient history printouts from the pharmacy that include required details. Make sure these documents contain:
Ensure all documentation is loose or taped to a separate sheet, avoiding staples or glue. Use the Reason for Claim Submission or Special Notes section for any additional comments. For further assistance, you may contact Express Scripts Customer Service at 1-800-451-6245. Finally, return the completed claim to the specified address provided on the form.
What is the purpose of the Express Scripts Fax form?
The Express Scripts Fax form is designed for you to submit prescription drug claims quickly and accurately. By filling out this form, you can ensure that your prescriptions are reviewed for coverage by your insurance plan. It allows you to provide all the necessary information needed to process your claim efficiently.
What information do I need to provide about the cardholder?
When filling out the form, you need to include details about the cardholder, who is typically the insured member. This includes the cardholder's name, date of birth, gender, ID number, address, telephone number, employer, and insurance carrier information. Make sure that the claim form is signed; unsigned forms cannot be processed.
How do I list patient information on the form?
You need to provide information for each patient who is submitting claims, including their name, relationship to the cardholder, gender, date of birth, and the number of prescriptions attached. Make sure to also include the pharmacy's name and address as well as the prescribing doctor’s name and DEA number for each patient listed.
What documentation should I include when submitting a claim?
It's essential to include prescription receipts or labels that detail the pharmacy name and address, date filled, drug name, strength and NDC, quantity, days supply, price, and the Rx number. Missing any of this information could lead to your claim being delayed or denied, so double-check your submissions!
Are there any specific instructions regarding receipts?
Yes! When submitting receipts, ensure they are unattached or taped to a separate piece of paper. Avoid stapling or gluing them, as this might complicate the processing of your claim. For a more efficient submission, feel free to include a patient history printout from your pharmacy, but remember that it must be signed by the dispensing pharmacist.
What should I do if I have questions about the form?
If you have any questions or concerns while filling out the Express Scripts Fax form, don't hesitate to reach out to Express Scripts' Customer Service Department at 1-800-451-6245. They can guide you through the process and address any specific queries you may have.
How do I submit the completed form?
Your completed form should be sent to Express Scripts, Inc. at the provided address: P.O. Box 66773, St. Louis, MO 63166-6773, Attention: Claims Department. Ensure that all required documentation is included for a smooth submission process.
Can I submit claims for diabetic supplies?
Absolutely! If your claim is for diabetic supplies, make sure to indicate this on the form. Provide the patient's name, the physician’s details, the type of supply (like lancets or syringes), and the relevant quantity of the supply. This information is crucial for proper processing.
Omitting Required Signatures: Many people forget to sign the claim form. An unsigned form cannot be processed and will be returned.
Incorrect Patient Information: Providing incorrect or incomplete patient details, such as name, relationship to the cardholder, or date of birth, can lead to delays.
Missing Prescription Receipts: Failure to attach the necessary pharmacy receipts or labels with required details may result in denial or return of the claim.
Not Using the Correct Format: Some individuals do not follow the specified format for printing names or other information, which can lead to confusion.
Checking Incorrect Boxes: Incorrectly marking the checkboxes for questions such as gender or whether the patient resides in an assisted living facility may cause errors in processing.
Failing to Provide Additional Notes: Not utilizing the “Reason for claim submission or special notes” section can result in crucial information being overlooked during processing.
When submitting a claim through the Express Scripts Fax form, there are several other important documents that might also be required. Each of these documents serves a specific purpose in facilitating a smooth claims process, ensuring that all necessary information is provided for review. Below is a list of common forms and documents often submitted alongside the Express Scripts Fax form:
Providing these documents can streamline the claims process, reducing the chances of delays or issues. Always check with the specific requirements of your insurance plan and Express Scripts for the most accurate and up-to-date information.
The Express Scripts Fax form shares similarities with the Medical Claims Form commonly used by healthcare providers for billing insurance companies. Both documents require detailed information about the patient, including their name, relationship to the cardholder, and date of birth. Additionally, each form necessitates the inclusion of pertinent medical details, such as the services rendered or medications prescribed. Proper signatures are essential on both forms to authorize the release of information to the respective insurance entity, ensuring compliance with both legal and privacy standards.
Another form that resembles the Express Scripts Fax form is the Health Insurance Claim Form (CMS-1500). This form is primarily used for submitting claims related to medical services rather than prescriptions, but the structure and required information are quite similar. It requires the patient's identifying information, the provider’s details, and a description of the services provided. Both forms necessitate accurate and complete information to avoid claim denials, emphasizing the importance of adherence to the guidelines set by the insurance carrier.
The Pharmacy Claim Form is yet another document similar to the Express Scripts Fax form. This form is specifically designed for filing pharmacy-related claims and requires similar information, such as the patient's data and prescription details. Both forms aim to compensate the provider for services rendered or medications dispensed. Moreover, they necessitate supporting documentation, such as receipts or labels, outlining the medication dispensed to ensure that the claim is processed accurately and swiftly.
Lastly, the Durable Medical Equipment (DME) Claim Form also shares characteristics with the Express Scripts Fax form. This document is used for claims related to medical equipment prescribed to patients. Like the Express Scripts form, it requires detailed patient information, a description of the equipment provided, and the provider's details. Both forms highlight the need for relevant prescriptions and supporting documentation to facilitate smooth processing of claims, serving to validate the medical necessity of the requested items.
When filling out the Express Scripts Fax form, it is essential to be meticulous. Here is a list of what you should and shouldn't do:
Completing the form correctly can prevent delays in your prescription claims. Pay close attention to each detail. If you have questions, reach out to customer service for assistance.
Misconceptions about the Express Scripts Fax form can lead to confusion. Addressing these misconceptions is essential for accurate claim submissions.
Clarifying these misconceptions can enhance the submission process for all involved.
Filling out the Express Scripts Fax form accurately is crucial for a smooth claims process. Here are key points to keep in mind:
Following these guidelines ensures a more efficient claim process with Express Scripts, minimizing potential issues or delays.