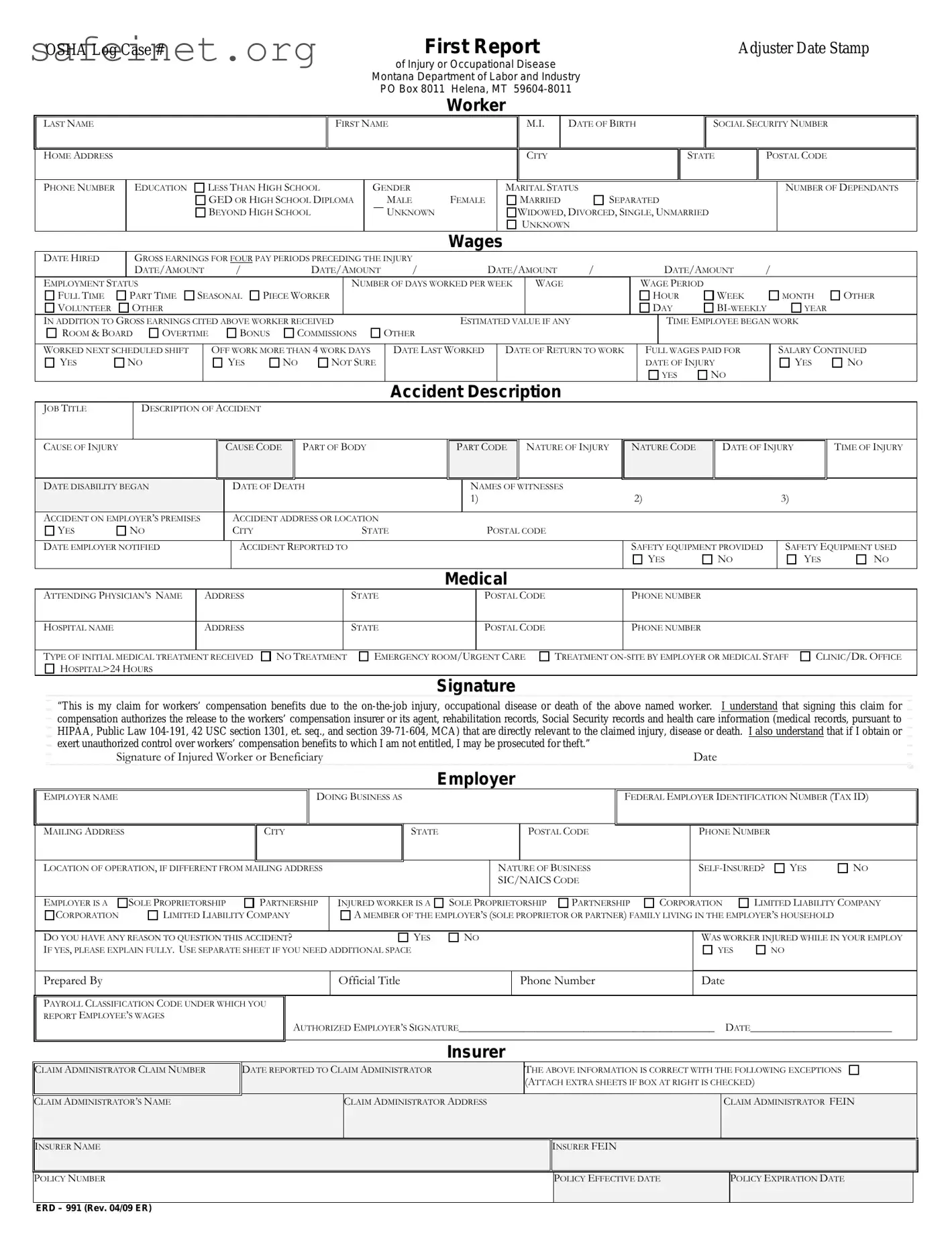
The ERD 991 form is a crucial part of the workers' compensation process in Montana. Designed for employees who have suffered work-related injuries or occupational diseases, this form captures vital information about the injured worker, the incident, and the employer’s details. It requires the injured worker to provide personal information such as their name, address, social security number, and employment status. Critical aspects also include details about the incident, like the date and cause of injury, job title, and a description of the accident itself. Employers are required to fill out sections regarding their operations, accident notifications, and insurance details. Medical treatment information, including the attending physician and the type of care received, is also documented. By signing the form, the injured worker authorizes the release of necessary records to support their claim. Accurate and timely completion of the ERD 991 is essential to ensure that workers receive the benefits they deserve without unnecessary delays.
OSHA Log Case #
First Report |
Adjuster Date Stamp |
of Injury or Occupational Disease
Montana Department of Labor and Industry PO Box 8011 Helena, MT
Worker
LAST NAME
HOME ADDRESS
FIRST NAME
M.I. |
DATE OF BIRTH |
|
|
CITY |
|
|
|
SOCIAL SECURITY NUMBER
STATE |
POSTAL CODE |
|
|
PHONE NUMBER
EDUCATION
LESS THAN HIGH SCHOOL
GED OR HIGH SCHOOL DIPLOMA
BEYOND HIGH SCHOOL
GENDER
MALE
UNKNOWN
FEMALE
MARITAL STATUS
MARRIED 
 SEPARATED
SEPARATED
WIDOWED, DIVORCED, SINGLE, UNMARRIED
UNKNOWN
NUMBER OF DEPENDANTS
Wages
|
DATE HIRED |
|
GROSS EARNINGS FOR FOUR PAY PERIODS PRECEDING THE INJURY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
|
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|
DATE/AMOUNT |
/ |
|
|
|||||||||||||
|
EMPLOYMENT STATUS |
|
|
|
|
|
|
|
|
|
|
|
NUMBER OF DAYS WORKED PER WEEK |
WAGE |
|
|
|
WAGE PERIOD |
|
|
|
|
|
|
|||||||||||
|
FULL TIME |
PART TIME |
SEASONAL |
PIECE WORKER |
|
|
|
|
|
|
|
|
|
|
|
|
|
HOUR |
|
WEEK |
|
|
MONTH |
OTHER |
|||||||||||
|
VOLUNTEER |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAY |
|
YEAR |
|
||||||
|
IN ADDITION TO GROSS EARNINGS CITED ABOVE WORKER RECEIVED |
|
|
|
|
ESTIMATED VALUE IF ANY |
|
|
|
|
TIME EMPLOYEE BEGAN WORK |
|
|||||||||||||||||||||||
|
ROOM & BOARD |
OVERTIME |
|
|
|
BONUS |
|
COMMISSIONS |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
WORKED NEXT SCHEDULED SHIFT |
|
|
OFF WORK MORE THAN 4 WORK DAYS |
|
DATE LAST WORKED |
|
DATE OF RETURN TO WORK |
|
FULL WAGES PAID FOR |
|
|
SALARY CONTINUED |
||||||||||||||||||||||
|
YES |
NO |
|
|
|
|
|
YES |
|
NO |
NOT SURE |
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF INJURY |
|
|
YES |
NO |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Accident Description |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
JOB TITLE |
|
DESCRIPTION OF ACCIDENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
CAUSE OF INJURY |
|
|
|
|
|
|
|
CAUSE CODE |
|
|
PART OF BODY |
|
|
|
PART CODE |
NATURE OF INJURY |
|
NATURE CODE |
|
DATE OF INJURY |
TIME OF INJURY |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE DISABILITY BEGAN |
|
|
|
|
|
|
DATE OF DEATH |
|
|
|
|
NAMES OF WITNESSES |
|
|
2) |
|
|
|
|
|
3) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
ACCIDENT ON EMPLOYER’S PREMISES |
|
|
|
ACCIDENT ADDRESS OR LOCATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
YES |
NO |
|
|
|
|
|
|
CITY |
|
|
|
|
STATE |
|
|
|
|
POSTAL CODE |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
DATE EMPLOYER NOTIFIED |
|
|
|
|
|
|
ACCIDENT REPORTED TO |
|
|
|
|
|
|
|
|
|
|
|
SAFETY EQUIPMENT PROVIDED |
|
|
SAFETY EQUIPMENT USED |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
NO |
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical
ATTENDING PHYSICIAN’S NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
PHONE NUMBER |
|
|
|
|
|
|
PHONE NUMBER |
HOSPITAL NAME |
ADDRESS |
|
STATE |
POSTAL CODE |
|
|
|
|
|
|
|
|
|
TYPE OF INITIAL MEDICAL TREATMENT |
RECEIVED |
NO TREATMENT |
EMERGENCY ROOM/U |
RGENT CARE |
TREATMENT ON |
|
HOSPITAL>24 HOURS |
|
|
|
|
|
|
CLINIC/DR. OFFICE
Signature
“This is my claim for workers’ compensation benefits due to the
Signature of Injured Worker or Beneficiary |
Date |
Employer
EMPLOYER NAME
DOING BUSINESS AS
FEDERAL EMPLOYER IDENTIFICATION NUMBER (TAX ID)
MAILING ADDRESS |
|
CITY |
|
STATE |
|
|
|
POSTAL CODE |
|
PHONE NUMBER |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
LOCATION OF OPERATION, IF DIFFERENT FROM MAILING ADDRESS |
|
|
|
NATURE OF BUSINESS |
|
YES |
NO |
||||||||
|
|
|
|
|
|
|
SIC/NAICS CODE |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
LIMITED LIABILITY COMPANY |
||||
EMPLOYER IS A |
SOLE PROPRIETORSHIP |
PARTNERSHIP |
INJURED WORKER IS A |
SOLE P |
ROPRIETORSHIP |
PARTNERSHIP |
CORPORATION |
||||||||
CORPORATION |
LIMITED LIABILITY COMPANY |
A MEMBER OF THE EMPLOYER’S (SOLE PROPRIETOR OR PARTNER) FAMILY LIVING IN THE EMPLOYER’S HOUSEHOLD |
|
||||||||||||
|
|
|
|
|
|
|
|
WAS WORKER INJURED WHILE IN YOUR EMPLOY |
|||||||
DO YOU HAVE ANY REASON TO QUESTION THIS ACCIDENT? |
|
YES |
NO |
|
|
||||||||||
IF YES, PLEASE EXPLAIN FULLY. USE SEPARATE SHEET IF YOU NEED ADDITIONAL SPACE |
|
|
|
|
|
|
YES |
NO |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Prepared By |
|
|
|
Official Title |
|
|
|
Phone Number |
|
Date |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PAYROLL CLASSIFICATION CODE UNDER WHICH YOU |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
REPORT EMPLOYEE’S WAGES |
|
AUTHORIZED EMPLOYER’S SIGNATURE_______________________________________________ |
DATE__________________________ |
||||||||||||
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurer
CLAIM ADMINISTRATOR CLAIM NUMBER
DATE REPORTED TO CLAIM ADMINISTRATOR
THE ABOVE INFORMATION IS CORRECT WITH THE FOLLOWING EXCEPTIONS (ATTACH EXTRA SHEETS IF BOX AT RIGHT IS CHECKED)
CLAIM ADMINISTRATOR’S NAME |
CLAIM ADMINISTRATOR ADDRESS |
|
CLAIM ADMINISTRATOR FEIN |
|
|
|
|
|
|
|
|
INSURER NAME |
|
INSURER FEIN |
|
|
|
|
|
|
|
|
|
POLICY NUMBER |
|
POLICY EFFECTIVE DATE |
|
POLICY EXPIRATION DATE |
|
|
|
|
|
|
|
ERD – 991 (Rev. 04/09 ER)
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The ERD 991 form serves as a claim for workers’ compensation benefits due to injuries, occupational diseases, or death related to work in Montana. |
| Governing Law | This form is governed by the Montana Workers’ Compensation Act, specifically under section 39-71 of the Montana Code Annotated (MCA). |
| Filing Requirements | The form must be filed with the Montana Department of Labor and Industry within specified timeframes after the injury occurs. |
| Signature Mandate | It requires the injured worker’s signature, which authorizes the release of pertinent medical and other records for the claim process. |
Completing the ERD 991 form is an essential step for filing a workers' compensation claim in Montana. This form gathers necessary personal, employment, and medical information regarding the worker and the incident, allowing the relevant parties to process the claim efficiently.
Carefully review the form for accuracy before submission to ensure proper handling of your claim.
What is the ERD 991 form used for?
The ERD 991 form is a document used to report workers' compensation claims related to on-the-job injuries or occupational diseases in Montana. It serves as the first report of injury and helps employers and insurance administrators process claims efficiently.
Who needs to fill out the ERD 991 form?
The injured worker, their employer, and the claim administrator should all be involved in filling out the ERD 991 form. This ensures accurate information is collected from all relevant parties for a complete claim process.
What information is required on the ERD 991 form?
The form requires personal details about the injured worker, such as their name, address, date of birth, and social security number. It also collects information related to the accident, job title, nature of the injuries, medical treatment received, and the employer's details.
How does the employer submit the ERD 991 form?
Employers can submit the ERD 991 form by mailing it to the Montana Department of Labor and Industry. The address is provided on the form. Timely submission is crucial for the processing of the workers’ compensation claim.
What should be included in the accident description section?
In the accident description section, provide a clear and concise account of how the injury or occupational disease occurred. Include relevant details like the job title, cause of injury, and a description of the accident to support the claim.
Can the injured worker decline to sign the ERD 991 form?
While it's possible for the injured worker to decline to sign, doing so may delay or complicate the claim process. Signing the form authorizes the release of necessary records, which is vital for the evaluation of the claim.
What happens after the ERD 991 form is submitted?
Once the ERD 991 form is submitted, the claim administrator will review the information. They will then determine the validity of the claim and communicate with the employer, the injured worker, and other relevant parties about the next steps.
Inconsistent Personal Information: Accurate and consistent information is crucial when filling out the Erd 991 form. Individuals often make the mistake of providing different names or inconsistent birth dates in multiple sections. This can lead to significant delays in processing claims.
Failure to Report All Earnings: Claimants sometimes overlook additional sources of income, such as overtime or bonuses. When filling out the gross earnings for the four pay periods preceding the injury, it’s essential to include all earnings. Failure to do so may result in a lower compensation claim.
Neglecting Medical Treatment Details: Adequate documentation of medical treatment is vital. Many forget to include the complete name or address of the attending physician or fail to specify the type of treatment received. Missing this information can complicate the evaluation of medical necessity and eligibility for benefits.
Inaccurate Accident Description: A clear and concise description of the accident is necessary for the claim's validity. Common errors include vague language or omitting important details regarding the cause of the injury. Providing accurate and thorough information can facilitate a smoother claims process.
Ignoring Signature Requirements: The form requires the injured worker or beneficiary's signature to validate the claim. Individuals often either forget to sign the document or fail to include the date of signature. This simple oversight can lead to an outright rejection of the claim.
The ERD 991 form is a critical document in processing workers' compensation claims. When completing this form, several other documents may also be necessary to ensure that the injury claim is handled appropriately. Below is a list of forms and documents that are often utilized alongside the ERD 991.
Employers, employees, and their representatives must ensure that these documents are correctly completed and submitted as needed. This will facilitate a smoother and more efficient claims process, aiding in the fair resolution of workplace injuries.
The ERD 991 form is notably similar to the workers' compensation claim form (WC-1), which serves a similar purpose in documenting details surrounding an employee's work-related injury or illness. Like the ERD 991, the WC-1 captures essential information such as the employee's personal details, the nature of the injury, and employer-related information. Both forms facilitate communication between the injured worker, the employer, and workers' compensation insurers. They aim to ensure that benefits are properly assessed and delivered, emphasizing the need for accuracy in reporting to expedite the claims process.
Another document akin to the ERD 991 is the OSHA Form 301, which is used to report work-related injuries and illnesses. This form collects comprehensive data on the event leading to an injury, including the location, nature of the accident, and involved employee's details. While the ERD 991 focuses more on the compensation aspect, OSHA Form 301 prioritizes safety and compliance in the workplace. Both forms aim to promote workplace safety by contributing to the overall understanding of workplace incidents and informing preventative measures.
The employee injury report is a further document that shares similarities with the ERD 991. Typically used by employers, this report captures the immediate details surrounding an accident, such as the date, time, and circumstances leading to an injury. Like the ERD 991, it serves as a formal record that both the employer and employee can refer to when pursuing a claim for benefits. The focus is on ensuring a detailed understanding of the incident to adhere to safety regulations and guidelines while also assisting in the compensation process.
Finally, the claim for disability benefits form resembles the ERD 991 in that it addresses an injured worker's need for financial compensation due to an inability to work. This form collects similar personal and employment details and assesses how the injury affects the individual’s ability to earn wages. While the ERD 991 primarily deals with workers' compensation claims, both forms underscore the importance of accurately documenting injury-related information to facilitate timely benefits and support for the affected worker.
Here are seven things to consider when filling out the ERD 991 form:
Filling out the Erd 991 form is crucial for initiating a workers’ compensation claim in Montana. Here are some important points to keep in mind:
Following these guidelines will help ensure that the Erd 991 form is properly completed and submitted without unnecessary delays in the claims process.