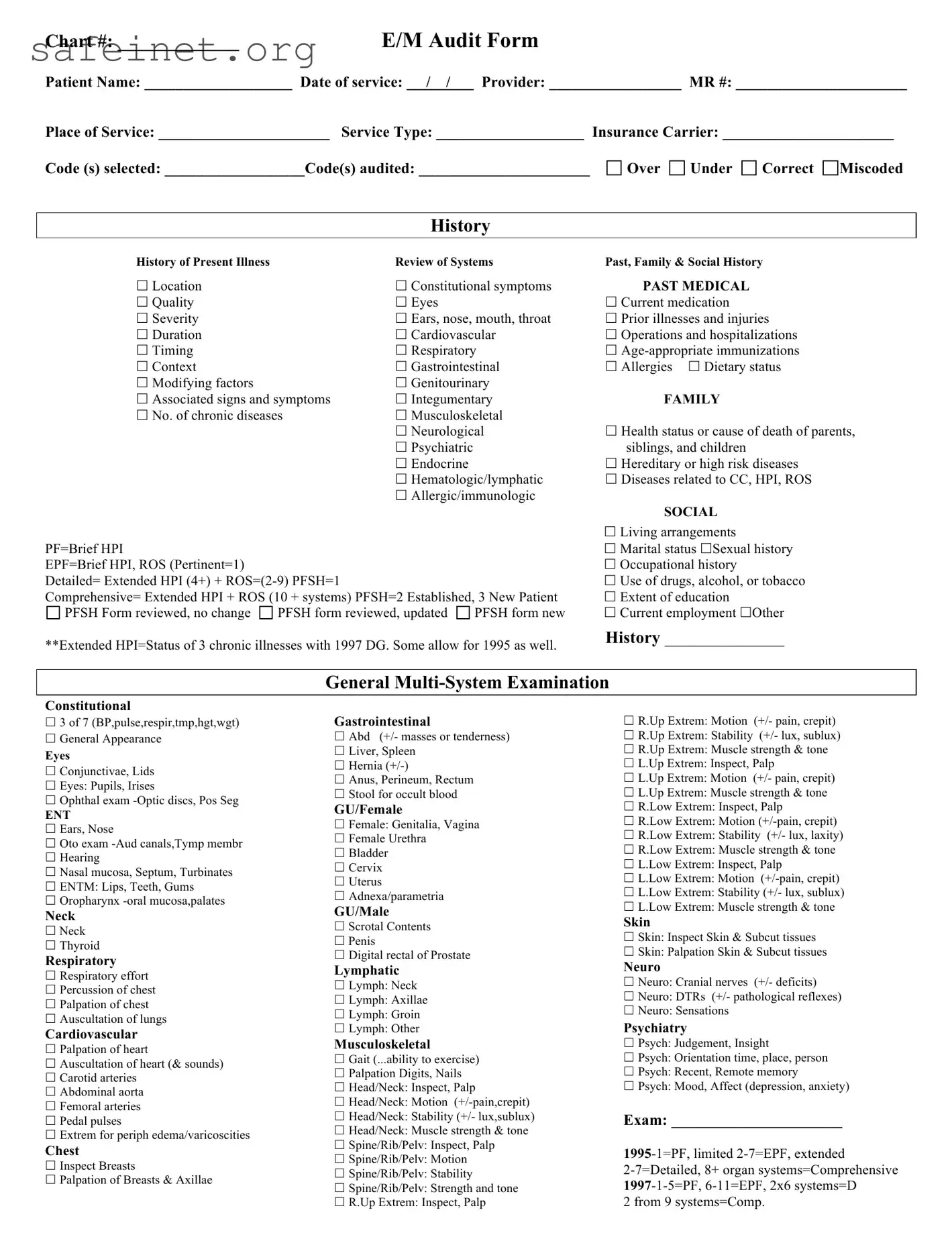
The E/M Audit form serves as a crucial tool in the evaluation of medical services offered during patient encounters. It encapsulates essential details including patient information, service date, provider identity, and place of service, among other vital data. Health care providers are required to make careful selections of coding options to ensure accurate billing and compliance. Critical components of this form focus on the assessment of a patient's history, physical examination, and the complexity of medical decision-making. Within the history section, providers document the history of present illness, past medical and surgical history, along with family and social history. A thorough physical examination adds further depth, covering multiple organ systems and their relevant characteristics. The form also prompts the auditor to categorize the level of complexity and risk associated with each patient's presenting problems, which can influence the coding outcomes significantly. Additionally, a systematic approach is encouraged through various checkboxes and fields, guiding the provider to ensure no pertinent areas are overlooked. Ultimately, the audit and coding process not only assists with proper reimbursement but also upholds the standards of care within the medical profession.
Chart #: _____________E/M Audit Form
Patient Name: ___________________ Date of service: __ / /__ Provider: _________________ MR #: ______________________
Place of Service: ______________________ Service Type: ___________________ Insurance Carrier: ______________________ |
||||
Code (s) selected: __________________Code(s) audited: ______________________ |
Over |
Under |
Correct |
Miscoded |
History
History of Present Illness |
|
Review of Systems |
Past, Family & Social History |
|
Location |
|
Constitutional symptoms |
PAST MEDICAL |
|
Quality |
|
Eyes |
|
Current medication |
Severity |
|
Ears, nose, mouth, throat |
Prior illnesses and injuries |
|
Duration |
|
Cardiovascular |
Operations and hospitalizations |
|
Timing |
|
Respiratory |
|
|
Context |
|
Gastrointestinal |
Allergies Dietary status |
|
Modifying factors |
|
Genitourinary |
|
|
Associated signs and symptoms |
Integumentary |
FAMILY |
||
No. of chronic diseases |
Musculoskeletal |
|
||
|
|
Neurological |
Health status or cause of death of parents, |
|
|
|
Psychiatric |
|
siblings, and children |
|
|
Endocrine |
|
Hereditary or high risk diseases |
|
|
Hematologic/lymphatic |
Diseases related to CC, HPI, ROS |
|
|
|
Allergic/immunologic |
|
|
|
|
|
|
SOCIAL |
|
|
|
|
Living arrangements |
PF=Brief HPI |
|
|
|
Marital status Sexual history |
EPF=Brief HPI, ROS (Pertinent=1) |
|
|
|
Occupational history |
Detailed= Extended HPI (4+) + |
|
|
Use of drugs, alcohol, or tobacco |
|
Comprehensive= Extended HPI + ROS (10 + systems) PFSH=2 Established, 3 New Patient |
Extent of education |
|||
PFSH Form reviewed, no change |
PFSH form reviewed, updated |
PFSH form new |
Current employment Other |
|
**Extended HPI=Status of 3 chronic illnesses with 1997 DG. Some allow for 1995 as well. |
History ______________ |
|
|
|
|
General |
|
|
|
Constitutional
3 of 7 (BP,pulse,respir,tmp,hgt,wgt)
General Appearance
Eyes
Conjunctivae, Lids
Eyes: Pupils, Irises
Ophthal exam
ENT
Ears, Nose
Oto exam
Hearing
Nasal mucosa, Septum, Turbinates
ENTM: Lips, Teeth, Gums
Oropharynx
Neck
Neck
Thyroid
Respiratory
Respiratory effort
Percussion of chest
Palpation of chest
Auscultation of lungs
Cardiovascular
Palpation of heart
Auscultation of heart (& sounds)
Carotid arteries
Abdominal aorta
Femoral arteries
Pedal pulses
Extrem for periph edema/varicoscities
Chest
Inspect Breasts
Palpation of Breasts & Axillae
Gastrointestinal
Abd (+/- masses or tenderness)
Liver, Spleen
Hernia
Anus, Perineum, Rectum
Stool for occult blood
GU/Female
Female: Genitalia, Vagina
Female Urethra
Bladder
Cervix
Uterus
Adnexa/parametria
GU/Male
Scrotal Contents
Penis
Digital rectal of Prostate
Lymphatic
Lymph: Neck
Lymph: Axillae
Lymph: Groin
Lymph: Other
Musculoskeletal
Gait (...ability to exercise)
Palpation Digits, Nails
Head/Neck: Inspect, Palp
Head/Neck: Motion
Head/Neck: Stability (+/- lux,sublux)
Head/Neck: Muscle strength & tone
Spine/Rib/Pelv: Inspect, Palp
Spine/Rib/Pelv: Motion
Spine/Rib/Pelv: Stability
Spine/Rib/Pelv: Strength and tone
R.Up Extrem: Inspect, Palp
R.Up Extrem: Motion (+/- pain, crepit)
R.Up Extrem: Stability (+/- lux, sublux)
R.Up Extrem: Muscle strength & tone
L.Up Extrem: Inspect, Palp
L.Up Extrem: Motion (+/- pain, crepit)
L.Up Extrem: Muscle strength & tone
R.Low Extrem: Inspect, Palp
R.Low Extrem: Motion
R.Low Extrem: Stability (+/- lux, laxity)
R.Low Extrem: Muscle strength & tone
L.Low Extrem: Inspect, Palp
L.Low Extrem: Motion
L.Low Extrem: Stability (+/- lux, sublux)
L.Low Extrem: Muscle strength & tone
Skin
Skin: Inspect Skin & Subcut tissues
Skin: Palpation Skin & Subcut tissues
Neuro
Neuro: Cranial nerves (+/- deficits)
Neuro: DTRs (+/- pathological reflexes)
Neuro: Sensations
Psychiatry
Psych: Judgement, Insight
Psych: Orientation time, place, person
Psych: Recent, Remote memory
Psych: Mood, Affect (depression, anxiety)
Exam: ______________________
2 from 9 systems=Comp.
|
|
Number of |
Points |
|
|
|
Diagnoses/Management Options |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
improved or worsening) |
|
|
|
|
Maximum 2 points in this |
|
|
|
|
category. |
|
|
|
|
|
|
|
|
|
Established problem (to |
1 |
|
|
|
examining MD); stable or |
|
|
|
|
improved |
|
|
|
|
|
|
|
|
|
Established problem (to |
2 |
|
|
|
examining MD); worsening |
|
|
|
|
|
|
|
|
|
New problem (to examining MD); |
3 |
|
|
|
no additional |
|
|
|
|
|
|
|
|
|
New problem (to examining MD); |
4 |
|
|
|
additional |
|
|
|
|
admit/transfer) |
|
|
|
|
|
|
|
|
|
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amount and/or Complexity of Data |
|
Points |
|
|
Reviewed |
|
|
|
|
|
|
|
|
|
Lab ordered and/or reviewed (regardless of # |
1 |
|
|
|
ordered) |
|
|
TABLE OF RISK
Level of |
Presenting Problem(s) |
Diagnostic Procedure(s) |
Management Options |
Risk |
|
Ordered |
Selected |
|
|
|
|
|
•One |
• Laboratory tests requiring |
• Rest |
|
cold, insect bite, tinea corporis |
venipuncture |
• Gargles |
|
|
• Chest |
• Elastic bandages |
|
|
• EKG/EEG |
• Superficial dressings |
|
|
• Urinalysis |
|
|
|
• Ultrasound, eg, echocardiography |
|
Minimal |
|
• KOH prep |
|
|
|
|
|
|
• Two or more |
• Physiologic tests not under stress, eg, |
• |
|
problems |
pulmonary function tests |
• Minor surgery with no identified risk |
|
• One stable chronic illness, eg, well |
• |
factors |
|
controlled hypertension, |
with contrast, eg, barium enema |
• Physical therapy |
|
dependent diabetes, cataract, BPH |
• Superficial needle biopsies |
• Occupational therapy |
|
• Acute uncomplicated illness or injury, |
• Clinical laboratory tests requiring |
• IV fluids without additives |
|
eg, cystitis, allergic rhinitis, simple |
arterial puncture |
|
Low |
sprain |
• Skin biopsies |
|
|
|
|
|
|
• One or more chronic illnesses with |
• Physiologic tests under stress, eg, |
• Minor surgery with identified risk factors |
|
mild exacerbation, progression, or side |
cardiac stress test, fetal contraction |
• Elective major surgery (open, |
|
effects of treatment |
stress test |
percutaneous or endoscopic) with no |
|
• Two or more stable chronic illnesses |
• Diagnostic endoscopies with no |
identified risk factors |
|
• Undiagnosed new problem with |
identified risk factors |
• Prescription drug management |
|
uncertain prognosis, eg, lump in breast |
• Deep needle or incisional biopsy |
• Therapeutic nuclear medicine |
|
• Acute illness with systemic symptoms, |
• Cardiovascular imaging studies with |
• IV fluids with additives |
|
eg, pyelonephritis, pneumonitis, colitis |
contrast and no identified risk factors, |
• Closed treatment of fracture or dislocation |
|
• Acute complicated injury, eg, head |
eg, arteriogram, cardiac |
without manipulation |
|
injury with brief loss of consciousness |
catheterization |
|
|
|
• Obtain fluid from body cavity, eg |
|
|
|
lumbar puncture, thoracentesis, |
|
Moderate |
|
culdocentesis |
|
|
|
|
|
|
|
|
|
|
1 |
|
|
ordered) |
|
|
|
|
|
Medicine section |
1 |
|
and/or reviewed |
|
|
|
|
|
Discussion of test results with performing |
1 |
|
physician |
|
|
|
|
|
Decision to obtain old record and/or obtain hx |
1 |
|
from someone other than patient |
|
|
|
|
|
Review and summary of old records and/or |
|
|
obtaining hx from someone other than patient |
2 |
|
and/or discussion with other health provider |
|
|
|
|
|
Independent visualization of image, tracing, or |
2 |
|
specimen (not simply review of report) |
|
|
|
|
|
Total |
|
|
|
|
High
•One or more chronic illnesses with severe exacerbation, progression, or side effects of treatment
•Acute or chronic illnesses or injuries that pose a threat to life or bodily function, eg, multiple trauma, acute MI, pulmonary embolus, severe respiratory distress, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failure
•An abrupt change in neurologic status, eg, seizure, TIA, weakness, sensory loss
•Cardiovascular imaging studies with contrast with identified risk factors
•Cardiac electrophysiological tests
•Diagnostic Endoscopies with identified risk factors
•Discography
•Elective major surgery (open, percutaneous or endoscopic) with identified risk factors
•Emergency major surgery (open, percutaneous or endoscopic)
•Parenteral controlled substances
•Drug therapy requiring intensive monitoring for toxicity
•Decision not to resuscitate or to de- escalate care because of poor prognosis
Medical Decision Making
Number of Diagnoses or Treatment Options
Amount and/or Complexity of Data to be Reviewed
Risk of Complications, Morbidity, Mortality

 MDM Level=2 out of 3
MDM Level=2 out of 3
SF
1
1
Minimal
LOW
2
2
Low
MOD
3
3
Moderate
HIGH
4
4
High
MDM ______________
Chart Note |
Comments |
Dictated |
Handwritten |
Form |
Illegible |
Note signed
Signature missing
Other Services or Modalities:
Auditor’s Signature
| Fact Name | Details |
|---|---|
| Purpose | The E/M Audit form is utilized to evaluate and ensure the accuracy and appropriateness of documentation related to Evaluation and Management (E/M) services provided to patients. |
| Patient Information | The form requires essential patient details such as name, date of service, and medical record number, which ensures that each audit is linked to the correct individual care record. |
| Compliance | The E/M coding process adheres to guidelines set by the Centers for Medicare & Medicaid Services (CMS) and the American Medical Association (AMA), establishing standards that must be followed to maintain compliance. |
| Data Points | The form includes a section for assessing and recording the complexity of medical decision-making, outlining various categories that reflect the nature of diagnoses, management options, and risks involved. |
| State-Specific Laws | For certain states, such as California, the governing laws include the California Business and Professions Code, which mandates record-keeping in accordance with medical standards and ethical considerations. |
To fill out the E/M Audit form accurately, gather all required patient and service information beforehand. Ensure you have details regarding the patient’s medical history, present illness, and any relevant examinations performed. This form helps in assessing the complexity and risk involved in the medical decision-making process for the patient's care.
Next, assess the patient's history. Mark the appropriate boxes based on the patient's medical details. This includes items like the History of Present Illness, Review of Systems, and Past Family & Social History. Be thorough in checking each aspect related to the patient’s current health conditions.
Once all sections are filled, review the form for any errors or missing information. Make sure everything is clear and legible. It is crucial for maintaining accurate records and facilitating effective patient care.
What is the purpose of the E/M Audit form?
The E/M Audit form serves as a structured tool for healthcare providers to evaluate and document the complexity and quality of patient visits. It helps ensure that the medical decision-making, history, and examination details align with the coding chosen for billing and reimbursement. This process is vital to maintain compliance with regulations and to optimize reimbursement for services provided.
How should I complete the form for each patient encounter?
To complete the form accurately, start by populating the basic patient information, including chart number, patient name, date of service, and provider details. Carefully document all relevant data pertaining to the patient's history, examination, and medical decision-making. Ensure that you check all applicable boxes concerning the history and examination components. Remember to select the correct codes that best reflect the services rendered, as this is critical for proper billing.
What is meant by 'History' in the context of the E/M Audit form?
The 'History' section evaluates the information gathered about the patient's current condition, past medical history, and relevant family and social backgrounds. It assesses the depth of the History of Present Illness (HPI), Review of Systems (ROS), and Past, Family, & Social History (PFSH). Each category is essential for creating a comprehensive view of the patient's health and informs the medical decision-making process.
What kind of details should be included in the ‘Examination’ section?
In the 'Examination' section, document findings from the patient’s physical examination in an organized manner. This includes constitutional checks (like vital signs), detailed examinations of various body systems (e.g., eyes, cardiovascular, gastrointestinal, musculoskeletal), and necessary neurological assessments. Aim to provide a thorough yet concise overview of significant findings that contribute to diagnosing the patient’s condition.
How does the form classify different levels of medical decision-making?
The E/M Audit form categorizes medical decision-making into various levels based on the complexity of diagnoses, amount and complexity of data to review, and the associated risks involved. These levels can range from minimal to high, helping auditors assess the appropriateness of the codes assigned based on the services rendered. Understanding these levels assists providers in evaluating the necessity of their actions and documentation.
What are the implications of incorrect coding on this form?
Incorrect coding can lead to several issues, including delayed or denied reimbursement from insurance companies. It may also expose healthcare providers to audits or compliance investigations. Overcoding can result in fines or penalties, while undercoding could mean lost revenue for services rendered. Accurate and thorough completion of the E/M Audit form helps mitigate these risks.
What should I do if I find that I have made an error on the form?
If you discover an error on the E/M Audit form, it's essential to address it promptly. Cross out the incorrect information, write the correct details clearly, and initial the change. Additionally, make a note of the change in the patient’s chart to ensure that there is a clear record of what was amended. This transparency will aid in any future reviews or audits.
Can the form be used for both established and new patients?
Yes, the E/M Audit form is suitable for both established and new patients. However, it is important to note that the criteria and documentation requirements may differ slightly for each category. When assessing new patients, providers typically need to gather more comprehensive information compared to established patients, as the latter will already have a medical history documented.
How do insurance companies utilize the information gathered in the E/M Audit form?
Insurance companies use the information from the E/M Audit form to determine if the billed services align with the documented patient care. They evaluate the documentation for accuracy, completeness, and appropriateness of the chosen codes. This assessment helps the insurers decide whether the care provided warrants payment and verifies that it adheres to established healthcare guidelines.
What resources can assist providers in learning more about properly using the E/M Audit form?
Providers can access a variety of resources to enhance their understanding of the E/M Audit form. These include coding manuals, online courses, webinars, and professional organizations that offer training on E/M coding guidelines. Collaboration with billing specialists and attending workshops can also provide practical knowledge and insights into effectively utilizing the form, leading to better compliance and more accurate billing practices.
Forgetting to fill in the Chart Number. This important detail helps streamline patient records.
Leaving the Patient Name section blank. It's vital to identify the patient accurately to avoid mix-ups.
Not providing the Date of Service. This date is crucial for tracking the timeline of patient care.
Misunderstanding the Service Type. Incorrect categorization can lead to billing issues or insurance disputes.
Neglecting to document Insurance Carrier details. This can result in denied claims or payment delays.
Incorrectly selecting the Codes without reviewing the service provided. This could lead to improper billing.
Failing to indicate the Code(s) audited. This oversight can create confusion during the audit process.
Omitting patient History details. A thorough history is essential for understanding the patient's condition.
Not ensuring the Exam section is completed. This part documents the clinical findings, which are critical for treatment planning.
Leaving clinical notes unsigned. A missing signature could raise questions about the authenticity of the documentation.
The E/M Audit Form serves as a vital tool in evaluating and ensuring accurate medical billing and coding for healthcare providers. Alongside it, various forms and documents are commonly used to capture critical information, maintain compliance, and streamline processes. Below is a list of supplementary documents often employed in conjunction with the E/M Audit Form.
Using these documents together with the E/M Audit Form enhances the effectiveness of patient care and ensures compliance with healthcare regulations. Each form plays a distinct role in the broader context of patient management and billing, contributing to a comprehensive healthcare administration process.
The E/M Audit form is similar to the Clinical Evaluation Document (CED), which is utilized to summarize patient consultations and examinations. Both documents focus on gathering patient history, current health conditions, and essential findings during appointments. They are structured to ensure a comprehensive understanding of the patient’s situation, highlighting critical areas like present illness and social history. The CED, like the E/M Audit form, provides a framework for providers to evaluate and document the necessity for interventions based on thorough assessments.
Another document akin to the E/M Audit form is the Patient Encounter Form (PEF). This form facilitates the documentation of patient visits, often focusing on the service rendered during a specific appointment. Similar to the E/M Audit form, the PEF captures necessary details such as patient demographics, visit reason, and relevant health information. Both forms serve to maintain a thorough record of patient interactions, ensuring that care decisions are informed by complete and accurate data.
The Progress Note shares similarities with the E/M Audit form in that it chronicles updates on patient care over time. Progress Notes contain assessments of ongoing issues, responding to previous visits while also detailing new findings. These notes, like the information gathered on the E/M Audit form, are crucial for establishing continuity of care and evaluating treatment efficacy, allowing healthcare providers to make informed decisions based on the evolution of a patient’s condition.
The Medical History Form (MHF) is another document that parallels the E/M Audit form. The MHF is used to compile a patient’s medical history, presenting critical information about past illnesses, surgeries, vaccinations, and family health backgrounds. Both documents prioritize accurate and detailed history-taking, which is essential for any medical evaluation. They facilitate a better understanding of the patient's health landscape and guide appropriate clinical decisions.
The Referral Form also shows similarities to the E/M Audit form, as it collects pertinent details to facilitate transitions between care providers. This form includes information on the patient's condition, reasons for referral, and relevant treatment history. Just like the E/M Audit form, the Referral Form aims to enhance communication and ensure that receiving providers have the necessary context to proceed with care effectively.
The Comprehensive Health Assessment (CHA) is comparable to the E/M Audit form in that it involves a holistic evaluation of a patient’s health status. The CHA includes detailed sections on medical history, lifestyle factors, and health behaviors. Both documents are structured to ensure that no critical health aspects are overlooked, ultimately facilitating thorough clinical evaluations and informed treatment planning.
Lastly, the Treatment Plan Document (TPD) has characteristics similar to the E/M Audit form in that it outlines recommended actions based on the assessment of a patient’s health. The TPD focuses on proposed treatments, goals, and follow-up measures. Both documents emphasize the importance of planning and proper documentation, helping to ensure that patient care is systematic and based on detailed evaluations that inform future strategies.
When filling out the Em Audit form, certain practices can enhance the accuracy and effectiveness of your submission. Below are key considerations to keep in mind:
This belief oversimplifies the purpose of the E/M Audit form. In reality, both new and established patients require accurate documentation to ensure appropriate coding and billing. Each patient encounter, regardless of their status, necessitates thorough quality checks through the E/M Audit process.
While billing is a significant aspect of the E/M Audit form, it also serves a crucial role in enhancing patient care. Documentation helps track patient history and treatment plans, leading to a more comprehensive understanding of individual patient needs and improving healthcare outcomes.
This misunderstanding overlooks the complexity of the evaluation and management process. The level of service is influenced by multiple factors, including the nature of the presenting problem, the amount of data reviewed, and the risk associated with the patient’s condition. Incorporating these factors is essential for accurately determining the appropriate level of service.
Although legal compliance is an aspect of documentation, the primary goal is to ensure continuity of care. Accurate documentation ensures that healthcare providers can make informed decisions about patient treatment, thus fostering better communication and coordination among the healthcare team.
Many may find the form intimidating at first glance; however, it is designed to streamline the documentation process when understood correctly. Using straightforward templates makes the form more approachable, allowing providers to focus on patient care rather than navigating complicated bureaucratic requirements.
While it can initially seem burdensome, implementing consistent documentation practices can significantly reduce time spent on the E/M Audit form in the long run. Training and familiarity with the form will lead to improved efficiency, ultimately benefiting both providers and patients.
Completing the E/M Audit form requires careful attention to detail in order to ensure proper evaluation and coding of medical services. Here are five key takeaways to consider while filling out and using this form:
By keeping these takeaways in mind, medical practitioners can effectively utilize the E/M Audit form to enhance coding practices and ensure compliant and accurate billing.