The ECERS Score Sheet form plays a key role in the process of immunization, specifically concerning the Hepatitis B vaccine in Texas. This form ensures that individuals receiving the vaccine, or their guardians, are fully informed about the vaccine, its risks and benefits, and their rights regarding personal health information. It facilitates informed consent, as it includes sections for personal details of the vaccine recipient, such as name, birthdate, and address. The form requires a clear acknowledgment that the recipient or authorized individual understands the necessity of the vaccine to prevent the disease it is aimed at. Additionally, it mandates a signature to affirm voluntary consent and includes detailed instructions for clinics regarding documentation of the vaccination process, covering manufacturer details and administration specifics. Privacy rights are also emphasized, ensuring individuals know they can access and amend their personal information as needed. This comprehensive approach adds layers of protection and clarity for both patients and providers, fostering a transparent and informed vaccination environment.
Texas Department of State Health Services
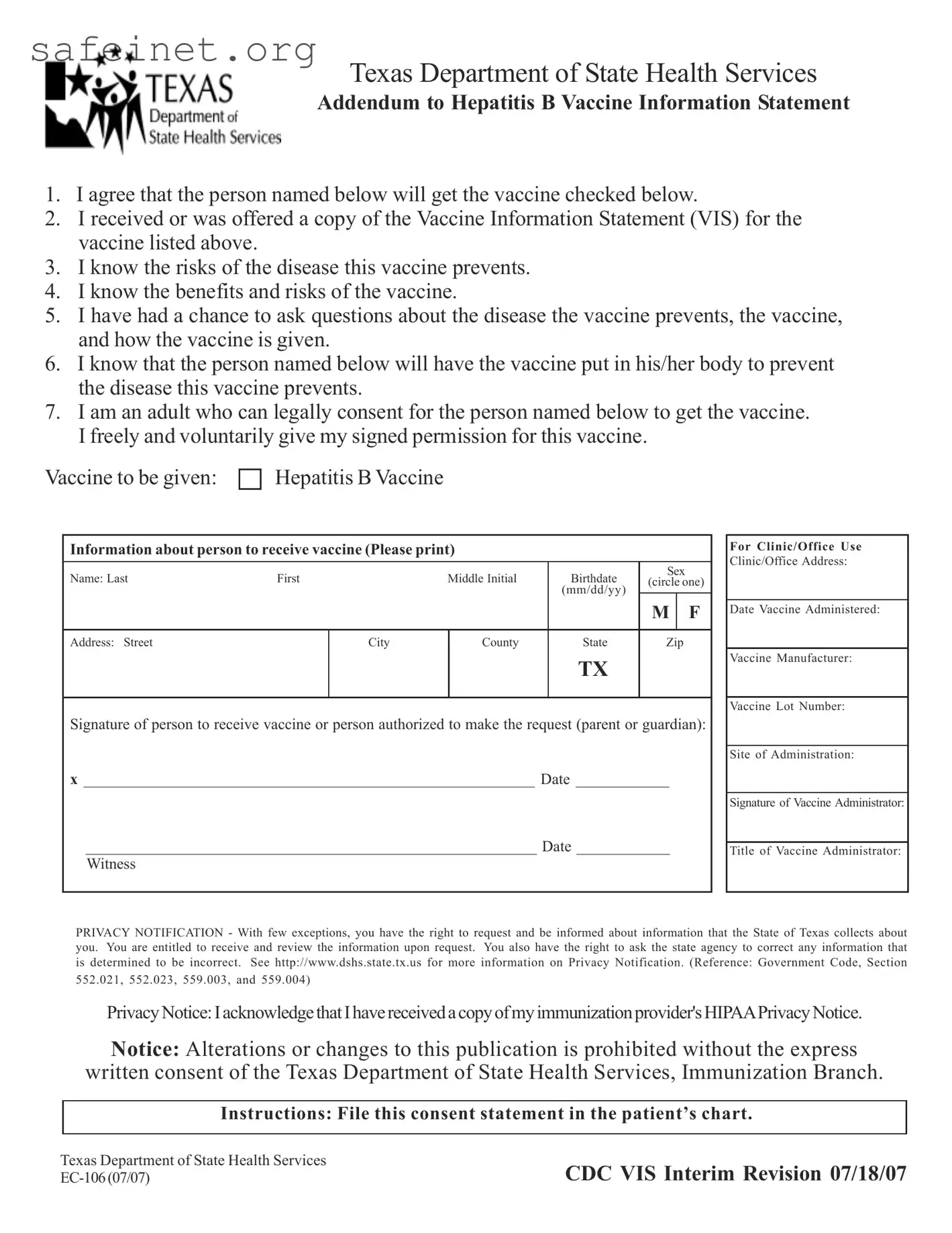
Addendum to Hepatitis B Vaccine Information Statement
1.I agree that the person named below will get the vaccine checked below.
2.I received or was offered a copy of the Vaccine Information Statement (VIS) for the vaccine listed above.
3.I know the risks of the disease this vaccine prevents.
4.I know the benefits and risks of the vaccine.
5.I have had a chance to ask questions about the disease the vaccine prevents, the vaccine, and how the vaccine is given.
6.I know that the person named below will have the vaccine put in his/her body to prevent the disease this vaccine prevents.
7.I am an adult who can legally consent for the person named below to get the vaccine. I freely and voluntarily give my signed permission for this vaccine.
Vaccine to be given:
Hepatitis B Vaccine
Information about person to receive vaccine (Please print)
Name: Last |
First |
Middle Initial |
Birthdate |
Sex |
|
||
(circle one) |
|||||||
|
|
|
(mm/dd/yy) |
||||
|
|
|
|
|
|
||
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
Address: Street |
City |
County |
State |
Zip |
|
||
TX
Signature of person to receive vaccine or person authorized to make the request (parent or guardian):
x __________________________________________________________ Date ____________
__________________________________________________________ Date ____________
Witness
For Clinic/Office Use
Clinic/Office Address:
Date Vaccine Administered:
Vaccine Manufacturer:
Vaccine Lot Number:
Site of Administration:
Signature of Vaccine Administrator:
Title of Vaccine Administrator:
PRIVACY NOTIFICATION - With few exceptions, you have the right to request and be informed about information that the State of Texas collects about you. You are entitled to receive and review the information upon request. You also have the right to ask the state agency to correct any information that is determined to be incorrect. See http://www.dshs.state.tx.us for more information on Privacy Notification. (Reference: Government Code, Section
552.021, 552.023, 559.003, and 559.004)
PrivacyNotice:IacknowledgethatIhavereceivedacopyofmyimmunizationprovider'sHIPAAPrivacyNotice.
Notice: Alterations or changes to this publication is prohibited without the express written consent of the Texas Department of State Health Services, Immunization Branch.
Instructions: File this consent statement in the patient’s chart.
Texas Department of State Health Services
CDC VIS Interim Revision 07/18/07
| Fact Name | Description |
|---|---|
| Vaccine Consent | The form requires consent for administering the Hepatitis B vaccine, ensuring informed agreement from the individual or legal guardian. |
| Information Statement | Individuals must acknowledge that they received or were offered the Vaccine Information Statement (VIS) related to the Hepatitis B vaccine. |
| Awareness of Risks | Signatories confirm they understand the risks associated with both the Hepatitis B disease and the vaccine itself. |
| Opportunity for Questions | The form indicates that individuals have had access to ask questions regarding the disease, vaccine, and its administration process. |
| Legal Age Requirement | The signer certifies they are a legal adult capable of providing consent for the vaccine on behalf of the individual receiving it. |
| Privacy Notification | Texas law (Government Code, Sections 552.021, 552.023, 559.003, and 559.004) outlines rights regarding personal data collected by the state. |
| Signature Requirement | A signature is required from the person receiving the vaccine or an authorized representative, providing legal acknowledgment of consent. |
| Witness Section | The form includes a section for a witness to validate the consent process, enhancing accountability and transparency. |
| Prohibition on Alterations | Any alterations to the publication are prohibited without written consent from the Texas Department of State Health Services. |
You are about to fill out the Ecers Score Sheet form. This process will help ensure all necessary information is collected for vaccine administration. Following these steps will make the completion straightforward and help maintain clarity.
Once completed, file the consent statement in the patient’s chart for future reference. Ensure all information is accurate and clearly legible to avoid complications.
What is the purpose of the Ecers Score Sheet form?
The Ecers Score Sheet form is designed to provide consent for the administration of the Hepatitis B vaccine. It ensures that the individual receiving the vaccine or their authorized representative understands the risks and benefits of the vaccine. Additionally, it serves as a documentation tool for healthcare providers to keep track of immunizations.
Who can sign the form for a minor?
An adult who has the legal right to make medical decisions for the minor, such as a parent or legal guardian, must sign the form. This ensures that the consent process complies with state regulations regarding vaccine administration.
What information must be provided on the form?
The form requires specific details, including the name and birthdate of the person receiving the vaccine, their address, and the signature of the person providing consent. Additional fields include the vaccine information, the clinic address, and the details of the vaccine administrator. This information helps in maintaining accurate vaccination records.
What happens if I want to change any information on the form?
Altering or changing the Ecers Score Sheet form is prohibited without the express written consent of the Texas Department of State Health Services. If you need to correct any information, it is best to contact your healthcare provider to ensure proper procedures are followed.
How does the Privacy Notification affect me?
The Privacy Notification informs you of your rights regarding the information collected about you by the state. You have the right to review this information and request corrections if necessary. This is part of the state's commitment to protecting your privacy and ensuring your data is accurate.
Not reading the entire form carefully: People often overlook key sections, which can lead to incomplete information.
Failing to provide accurate personal information: Some may misspell names or provide incorrect birthdates, causing delays in processing.
Overlooking the consent signature: A signature is essential. Without it, the form cannot be considered valid.
Ignoring the witness requirement: Some individuals forget to include a witness, which can also affect the form’s acceptance.
Not checking contact information: Providing an inaccurate address can hinder communication regarding the vaccination.
Missing date entries: Dates need to be provided, especially for consent and administration. Omitting these can create confusion.
Neglecting to circle the sex of the recipient: This detail is necessary and should not be skipped.
Forgetting to indicate the vaccine details: Specific information about the vaccine, such as the manufacturer and lot number, is critical for record-keeping.
The ECERS Score Sheet form plays a crucial role in evaluating the quality of early childhood programs. To support the completion and understanding of this score sheet, a variety of additional forms and documents may be utilized. Each serves a specific purpose, contributing to sound decision-making and informed consent processes.
These documents work together to create a comprehensive system that ensures informed consent, proper record-keeping, and adherence to legal and ethical standards. Each form not only facilitates communication between healthcare providers and patients but also safeguards public health through meticulous vaccination practices.
The Vaccine Administration Record (VAR) serves a similar purpose to the Ecers Score Sheet. Both documents ensure proper consent for vaccine administration. They require clear identification of the person receiving the vaccine, as well as the individual providing consent. The VAR records important details such as vaccine type, administration date, and administering personnel. Like the Ecers Score Sheet, the VAR offers a space for questions, ensuring that the recipient or guardian is fully informed about the vaccine’s risks and benefits.
The Immunization Consent Form is another document akin to the Ecers Score Sheet. This form also collects essential patient information and informs the signer about the vaccine administered. It emphasizes the importance of understanding the benefits and risks associated with immunization. The person giving consent, typically a parent or guardian for minors, must sign it, just as they do with the Ecers Score Sheet. Both forms are vital for legal and health compliance in documenting consent for vaccinations.
The Patient Information Sheet (PIS) resembles the Ecers Score Sheet in that it provides background information about the vaccine and the disease it aims to prevent. The PIS outlines potential side effects and the importance of the vaccination. It serves to educate patients or guardians and must be reviewed before signing any consent form. As with the Ecers Score Sheet, it reinforces informed decision-making regarding health and wellness.
The Medication Administration Record (MAR) shares similarities with the Ecers Score Sheet by tracking consent and administration of a specific treatment. While the Ecers focuses on vaccines, the MAR can apply to other medications. Both documents require details about the individual receiving treatment, consent by a responsible party, and verification of the administration process. This ensures that the individual’s healthcare history is accurately documented and that proper procedures are followed.
The Health History Form also aligns with the Ecers Score Sheet as it gathers critical information about the patient. It often includes past vaccinations, allergies, and medical conditions. This form aids healthcare providers in making informed decisions about the patient’s care and vaccination needs. By ensuring a comprehensive understanding of the patient’s health status, both forms promote safety and efficacy in healthcare delivery.
Lastly, the Consent for Treatment Form mirrors the Ecers Score Sheet in structure and intent. It seeks permission from patients or guardians before administering any medical treatment, including vaccinations. Both forms emphasize informed consent and require signatures from authorized individuals. They play a crucial role in medical practice, ensuring transparency and accountability in the healthcare process.
When filling out the Ecers Score Sheet form, it's essential to keep some key points in mind to ensure the process goes smoothly. Here’s a list of things you should and shouldn’t do.
By following these guidelines, you can confidently complete the Ecers Score Sheet form without unnecessary issues. Attention to detail and understanding the requirements are key to a great experience.
Misunderstandings about the Ecers Score Sheet form can lead to confusion when it comes to vaccine administration. Here’s a look at some common misconceptions surrounding this important document.
Understanding these misconceptions helps clarify the role and importance of the Ecers Score Sheet form in vaccine administration. Always feel encouraged to ask questions and seek clarity about any part of the process, as informed consent is key to ensuring health and safety.
The Ecers Score Sheet form serves an important purpose in the vaccination process. Here are key takeaways to consider: