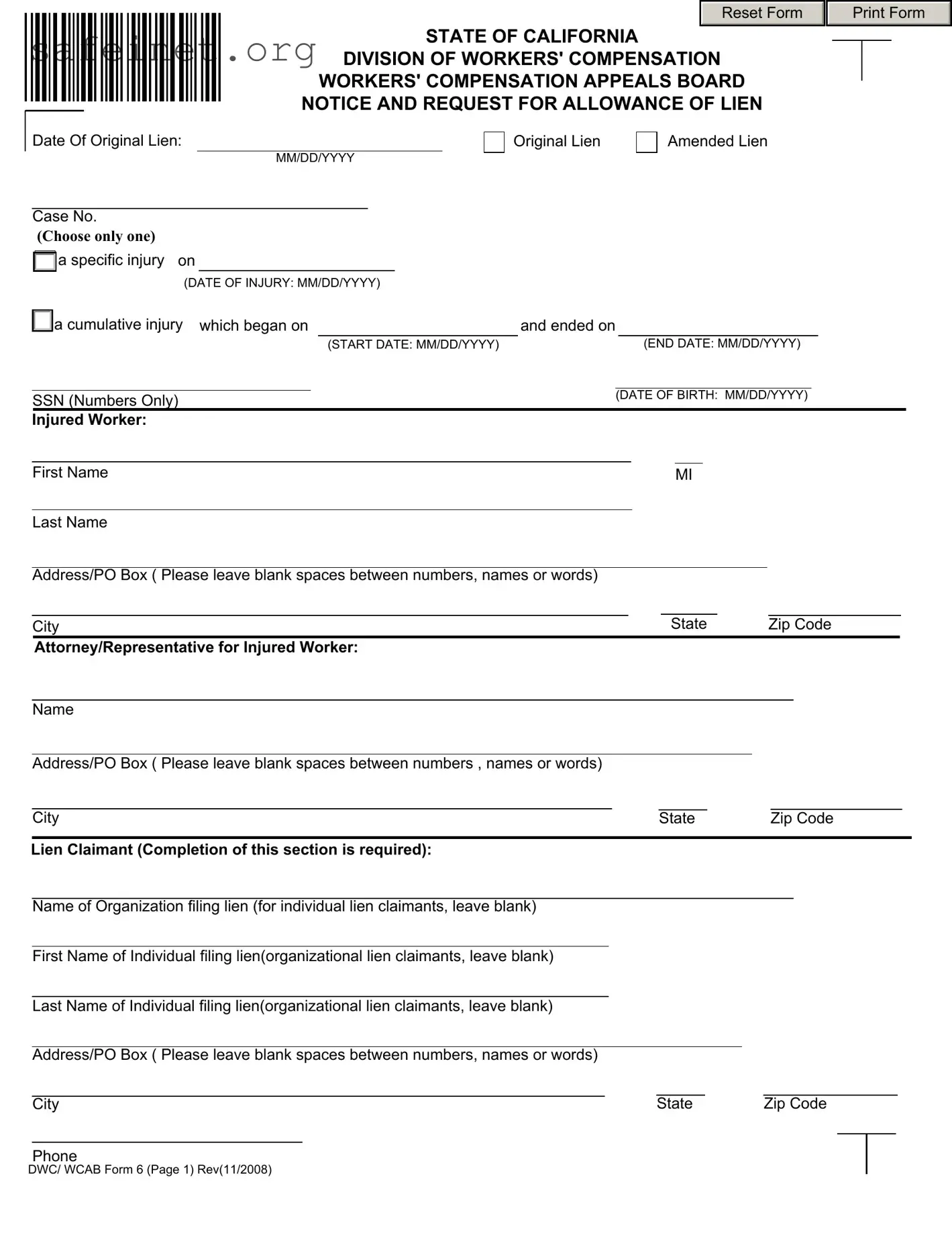
The DWC WCAB 6 form plays a crucial role in California’s workers' compensation system, specifically addressing the process of filing a lien. This form allows lien claimants—those who believe they are owed money related to an injured worker's claim—to formally request a review by the Workers’ Compensation Appeals Board. It encompasses various essential details such as the dates of injury, the nature of the claim, and the parties involved, ensuring that all required information is accurately captured. The form prompts lien claimants to specify the amount they are seeking, which can include not only attorney’s fees but also medical expenses and living costs incurred due to the injury. Liability is a key consideration, as the board must determine if these expenses are valid under California's labor laws. By submitting this form, the lien claimant can assert their rights and obligations, facilitating a fair resolution in the workers' compensation process. Understanding the components and significance of the DWC WCAB 6 form can empower injured workers and their representatives as they navigate these often complex legal waters.
Reset Form
STATE OF CALIFORNIA 
 DIVISION OF WORKERS' COMPENSATION
DIVISION OF WORKERS' COMPENSATION
WORKERS' COMPENSATION APPEALS BOARD
NOTICE AND REQUEST FOR ALLOWANCE OF LIEN
Print Form
Date Of Original Lien:
MM/DD/YYYY
Case No.
(Choose only one)

 a specific injury on
a specific injury on
(DATE OF INJURY: MM/DD/YYYY)

 Original Lien
Original Lien
Amended Lien
a cumulative injury which began on |
and ended on |
||
|
(START DATE: MM/DD/YYYY) |
|
(END DATE: MM/DD/YYYY) |
SSN (Numbers Only)
Injured Worker:
(DATE OF BIRTH: MM/DD/YYYY)
|
First Name |
|
|
|
|
|
MI |
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address/PO Box ( Please leave blank spaces between numbers, names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
City |
|
|
|
|
State |
|
|
Zip Code |
|
||||||||||||||
|
Attorney/Representative for Injured Worker: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address/PO Box ( Please leave blank spaces between numbers , names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
City |
|
State |
|
|
|
Zip Code |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lien Claimant (Completion of this section is required): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Organization filing lien (for individual lien claimants, leave blank) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name of Individual filing lien(organizational lien claimants, leave blank) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Last Name of Individual filing lien(organizational lien claimants, leave blank) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Address/PO Box ( Please leave blank spaces between numbers, names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
City |
|
|
State |
|
Zip Code |
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
DWC/ WCAB Form 6 (Page 1) Rev(11/2008)
|
|
Lien Claimant's Attorney/Representative, if any |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Law Firm/Attorney |
Lien Claimant not represented |
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lien Claimant Law Firm/Representative |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address/PO Box ( Please leave blank spaces between numbers, names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
State |
Zip Code |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address/PO Box ( Please leave blank spaces between numbers, names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Zip Code |
|
||||||||||||||
|
|
City |
|
|
|
|
|
|
State |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance Carrier or Claims Administrator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address/PO Box ( Please leave blank spaces between numbers, names or words) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
City |
|
|
|
|
|
|
|
State |
|
Zip Code |
|
|
||||||||
Employer or Claims Administrator Attorney/Representative (if known)
Name
Address/PO Box ( Please leave blank spaces between numbers, names or words)
|
|
|
|
Zip Code |
City |
State |
DWC/ WCAB Form 6 (Page 2) Rev(11/2008)
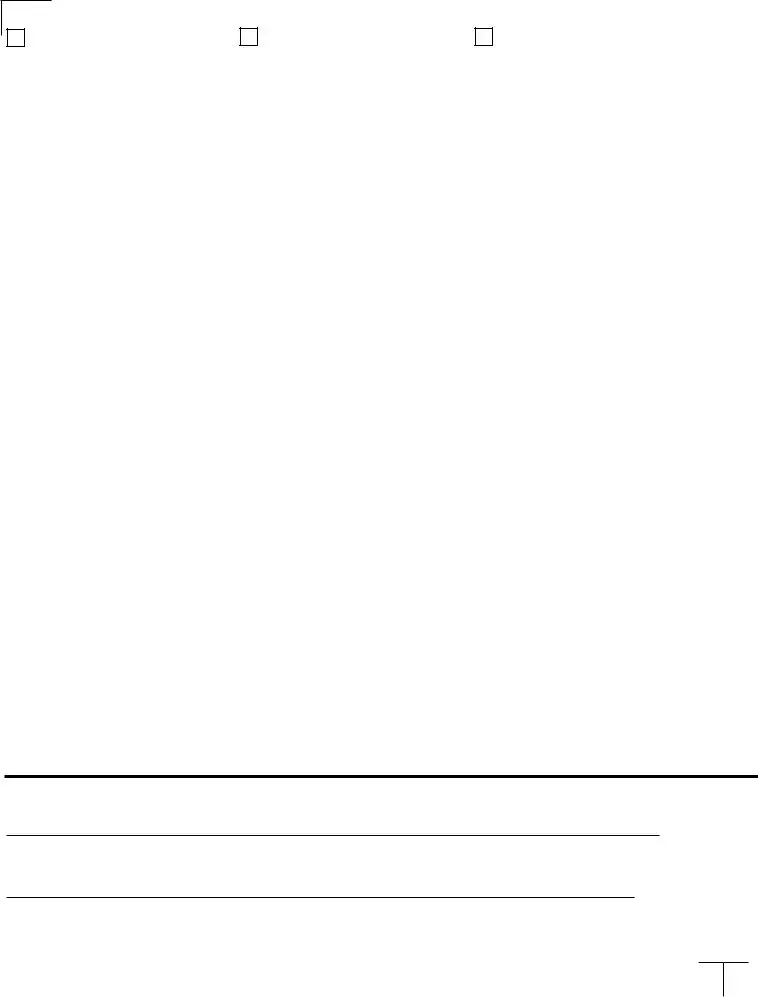
The lien claimant hereby requests the Workers' Compensation Appeals Board to determine and allow as a lien the sum
of $ |
against any amount now due or which may hereafter become payable as |
Total Lien Amount
compensation to the
This request and claim for lien is for (mark appropriate box):
A reasonable attorney's fee for legal services pertaining to any claim for compensation either before the appeals board or before any of the appellate courts, and the reasonable disbursements in connection therewith. (Labor Code § 4903 (a).)
The reasonable expense incurred by or on behalf of the injured employee, as provided by Labor Code § 4600. (Labor Code § 4903 (b).)
Reasonable expense incurred by or on behalf of the injured employee for
The reasonable value of the living expenses of an injured employee or of his or her dependents, subsequent to the injury. (Labor Code § 4903 (c).)
The reasonable burial expenses of the deceased employee. (Labor Code § 4903 (d).)
The reasonable living expenses of the spouse or minor children of the injured employee, or both, subsequent to the date of the injury, where the employee has deserted or is neglecting his or her family. (Labor Code § 4903 (e).)
The reasonable fee for interpreter's services performed on |
|
20 |
|
. (Labor Code § 4600 (f).) |
The amount of indemnification granted by the California Victims of Crime Program. (Labor Code § 4903 (i).)
The amount of compensation, including expenses of medical treatment, and recoverable costs that have been paid by the Asbestos Workers' Account. (Labor Code § 4903 (j).)
Other Lien(s): Specify nature and statutory basis.
NOTE: ITEMIZED STATEMENT JUSTIFYING THE LIEN MUST BE ATTACHED

 A copy of the lien claim and supporting documents was served by mail or delivered to each of the
A copy of the lien claim and supporting documents was served by mail or delivered to each of the
|
|
|
|
|
(Signature of Attorney/Representative for Lien Claimant) |
(Signature of Lien Claimant) |
Date (MM/DD/YYYY) |
||
DWC/ WCAB Form 6 (Page 3) Rev(11/2008)
| Fact Name | Details |
|---|---|
| Purpose of the Form | The DWC WCAB 6 form is used to request the allowance of a lien for various costs related to a workers' compensation claim. |
| Governing Law | This form is governed by California Labor Code, specifically sections 4903 and 4600. |
| Filing Requirements | The lien claimant must provide an itemized statement justifying the lien and serve a copy of the claim to all relevant parties. |
| Types of Claims | The form allows for multiple types of claims, including attorney’s fees, medical expenses, and living or burial expenses. |
| Form Revision Date | The current version of the DWC WCAB 6 form was revised in November 2008. |
After preparing the form, follow these clear steps to ensure it is filled out correctly. Completing the DWC WCAB 6 form accurately is essential for it to be processed without delays.
What is the purpose of the DWC WCAB 6 form?
The DWC WCAB 6 form is used to request the Workers' Compensation Appeals Board to recognize and allow a lien for expenses related to workers' compensation claims. This may include attorney fees, medical expenses, or other related costs incurred on behalf of the injured worker.
Who should file the DWC WCAB 6 form?
The form should be filed by lien claimants, which can include attorneys, medical providers, or organizations that have provided services or benefits to the injured worker and are seeking reimbursement from the workers' compensation benefits awarded.
What information is required to complete the DWC WCAB 6 form?
Completion of the form requires details such as the date of the original lien, case number, injured worker’s information, lien claimant’s information, and a total lien amount. Additionally, you must indicate the type of expenses being claimed, selecting the appropriate box that matches your situation.
Can I amend a previously filed lien using the DWC WCAB 6 form?
Yes, if you need to amend a previously filed lien, you can indicate that on the form. Make sure to provide the updated information and explanation for the amendment as required by the filing instructions.
Is there a deadline for filing the DWC WCAB 6 form?
Timely filing is crucial in workers' compensation cases. While specific deadlines can vary based on the case, it’s generally advisable to submit the lien as soon as relevant expenses have been incurred or services rendered. Check with relevant authorities for specific deadlines that may apply to your situation.
What happens after I submit the DWC WCAB 6 form?
Once the form is submitted, the Workers' Compensation Appeals Board will review the claim. An order will be issued that determines whether the lien is allowed. All involved parties, including the injured worker and employer, will be notified of the decision.
What should I do if my lien is disputed?
If your lien is disputed, you may need to provide further documentation to support your claim. It may also be necessary to attend a hearing before the Workers' Compensation Appeals Board. Consulting with a legal professional can help you navigate this process effectively.
Inaccurate Dates: Filling in incorrect dates for the injury or the lien can lead to complications. Ensure all dates are properly formatted and accurate.
Incomplete Information: Failing to provide all required information can delay the processing of the form. Pay attention to each section and fill it out completely.
Incorrect Contact Details: Providing wrong phone numbers or addresses for parties involved may hinder communication. Double-check all contact information for accuracy.
Missing Signatures: Forgetting to sign the form can invalidate your request. Both the lien claimant and their attorney must provide the necessary signatures.
Failure to Attach Supporting Documents: Not including the required itemized statement or other supporting documents can result in rejection of the lien claim. Make sure all documents are attached as required.
Choosing the Wrong Case Type: Selecting the incorrect type of lien (original or amended) can complicate the process. Review your case type and mark the appropriate box accurately.
The DWC WCAB 6 form is a key document used in the workers' compensation process, specifically for lien claims in California. Several other forms and documents are typically utilized alongside the DWC WCAB 6 form to ensure that all relevant information is properly gathered and processed. Below is a list of commonly associated forms and documents.
These additional documents play an essential role in the workers' compensation process. By ensuring that all necessary information is collected and presented, they help facilitate a smoother resolution and aid in protecting the rights of injured workers and lien claimants alike.
The DWC WCAB 6 form is often compared to the DWC WCAB 1 form, which serves as a notice of claim form. Much like the DWC WCAB 6 form, the DWC WCAB 1 document is used to initiate a request regarding benefits associated with a work-related injury. While the DWC WCAB 6 focuses on the allowance of a lien related to medical or legal expenses, the DWC WCAB 1 tends to address the initial claim for benefits, providing an opportunity for injured workers to communicate their need for compensation directly to the Workers' Compensation Appeals Board.
Another similar document is the DWC WCAB 2 form, which is a request for adjustments or changes to existing liens or claims. This form, like the DWC WCAB 6, facilitates the dialogue between injured workers and the appeals board regarding financial claims. While the DWC WCAB 6 details specific liens, the DWC WCAB 2 allows for corrections or modifications in previously submitted claims, ensuring that all parties have the most current information regarding their requests for compensation.
The DWC WCAB 10 form, also known as the Declaration of Readiness to Proceed, shares similarities with the DWC WCAB 6 form in that it is part of the litigation process related to workers' compensation claims. While the DWC WCAB 6 is used to claim a lien, the DWC WCAB 10 is utilized to indicate readiness for a hearing regarding the underlying claim. Both documents aim to streamline communication and resolve issues surrounding claims, although they serve distinct roles in the process.
An additional form, the DWC WCAB 22, can also be likened to the DWC WCAB 6. The DWC WCAB 22 is used to file an application for adjudication of a claim. Much like the DWC WCAB 6, this form enables either party to present their case before the appeals board. The process for both forms necessitates thorough adherence to stipulations regarding submissions and serving notice to all relevant parties involved in the claims process.
The DWC WCAB 14 form, which is a lien conference statement, parallels the DWC WCAB 6 form through its emphasis on addressing lien claims. The DWC WCAB 14 provides a framework for detailing disputed issues related to liens, whereas the DWC WCAB 6 is a formal request for lien allowance based on expenses or fees incurred. Both forms aim to establish clarity regarding financial claims resulting from workers' compensation cases.
Similarly, the DWC WCAB 15, which is used to dispute or respond to a lien claim, also has a connection to the DWC WCAB 6 form. While the DWC WCAB 6 seeks to establish a claim for lien allowance, the DWC WCAB 15 functions as a response to potential conflicts surrounding that claim. This interaction is crucial in ensuring all claims are fairly evaluated and resolved, highlighting the importance of documentation in the appeals process.
The last document to mention in connection with the DWC WCAB 6 form is the DWC WCAB 13 form, which is used for settlements involving lien claims. In a similar vein, the DWC WCAB 6 outlines the expenses for which the lien claimant seeks repayment. The DWC WCAB 13 serves as a tool for resolving disputes by establishing a formal settlement process for those lien claims, ultimately aiding in the expedient resolution of financial obligations arising from work-related injuries.
When completing the DWC WCAB 6 form, it is crucial to adhere to certain guidelines to ensure accuracy and compliance. Below is a list of what you should and should not do in this process.
Attention to these guidelines will help streamline the review process and minimize potential issues with your lien request.
When it comes to the DWC WCAB 6 form, several misconceptions can lead to confusion. Understanding these myths is crucial for anyone involved in the workers' compensation process. Here’s a breakdown of nine common misconceptions:
By dispelling these misconceptions, individuals can better navigate the complexities surrounding the DWC WCAB 6 form and the workers' compensation system as a whole. Awareness and understanding are key to achieving a favorable outcome.