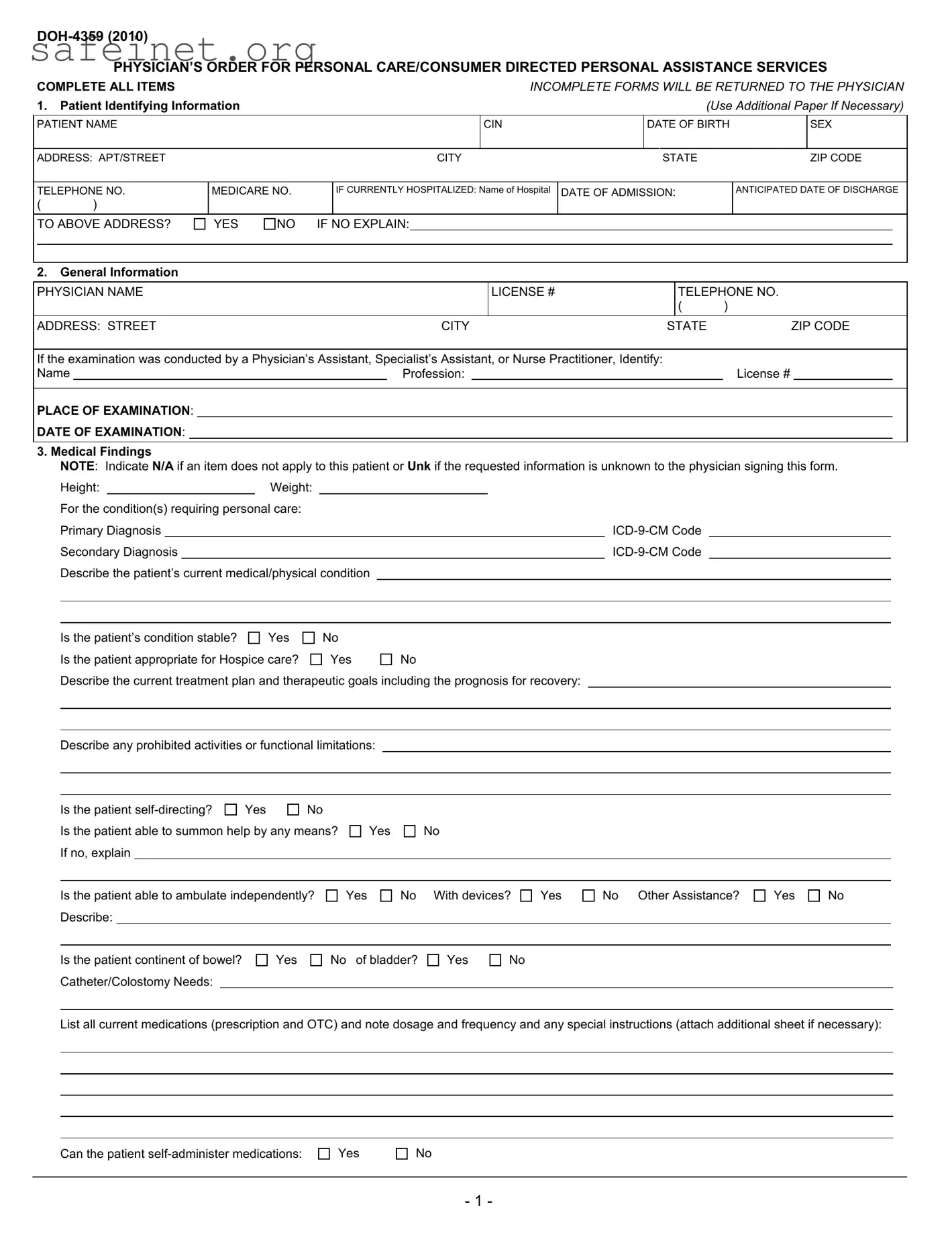
The DOH-4359 form, officially known as the Physician's Order for Personal Care/Consumer Directed Personal Assistance Services, plays a crucial role in facilitating home care for patients in need. This document ensures that healthcare providers can accurately communicate vital patient information to the New York State Department of Health, enabling the proper allocation of assistance services. It prompts physicians to detail essential details, such as the patient's identifying information, medical condition, and the need for personal care. The form covers a range of factors including diagnoses, treatment plans, and the patient’s ability to perform daily activities. Additionally, it gathers insights regarding the patient's stability, nutritional needs, and any required assistance with skilled tasks, such as glucose monitoring or medication administration. By covering these key aspects, the DOH-4359 not only helps streamline the process for patients receiving needed support but also ensures compliance with state regulations, thereby protecting both the patient's rights and the healthcare provider's responsibilities.
PHYSICIAN’S ORDER FOR PERSONAL CARE/CONSUMER DIRECTED PERSONAL ASSISTANCE SERVICES
COMPLETE ALL ITEMS |
|
|
|
|
|
|
|
|
|
|
INCOMPLETE FORMS WILL BE RETURNED TO THE PHYSICIAN |
||||||||||||||||||||||
1. |
Patient Identifying Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Use Additional Paper If Necessary) |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
PATIENT NAME |
|
|
|
|
|
|
|
|
|
CIN |
|
|
|
DATE OF BIRTH |
|
|
SEX |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS: APT/STREET |
|
|
|
|
|
|
|
CITY |
|
|
|
STATE |
|
|
|
|
|
ZIP CODE |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
TELEPHONE NO. |
MEDICARE NO. |
|
|
IF CURRENTLY HOSPITALIZED: Name of Hospital |
DATE OF ADMISSION: |
|
|
|
ANTICIPATED DATE OF DISCHARGE |
||||||||||||||||||||||||
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
TO ABOVE ADDRESS? |
YES |
NO |
IF NO EXPLAIN: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
General Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
PHYSICIAN NAME |
|
|
|
|
|
|
|
|
|
|
LICENSE # |
|
|
|
|
TELEPHONE NO. |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
ADDRESS: STREET |
|
|
|
|
|
|
|
CITY |
|
|
|
STATE |
ZIP CODE |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
If the examination was conducted by a Physician’s Assistant, Specialist’s Assistant, or Nurse Practitioner, Identify: |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Name |
|
|
|
|
|
|
|
Profession: |
|
|
|
|
|
|
|
|
|
License # |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PLACE OF EXAMINATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
DATE OF EXAMINATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
3. Medical Findings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
NOTE: Indicate N/A if an item does not apply to this patient or Unk if the requested information is unknown to the physician signing this form. |
|||||||||||||||||||||||||||||||
|
|
Height: |
|
|
Weight: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
For the condition(s) requiring personal care: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Primary Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Secondary Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Describe the patient’s current medical/physical condition |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Is the patient’s condition stable? |
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Is the patient appropriate for Hospice care? |
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
Describe the current treatment plan and therapeutic goals including the prognosis for recovery: |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Describe any prohibited activities or functional limitations:
Is the patient |
Yes |
No |
Is the patient able to summon help by any means? If no, explain
Yes
No
Is the patient able to ambulate independently? Describe:
Yes
No With devices?
Yes
No Other Assistance?
Yes
No
Is the patient continent of bowel? Catheter/Colostomy Needs:
Yes
No of bladder?
Yes
No
List all current medications (prescription and OTC) and note dosage and frequency and any special instructions (attach additional sheet if necessary):
Can the patient
Yes
No
- 1 -
If the patient requires a modified diet or has other special nutritional or dietary needs, describe:
Please indicate any task, treatments or therapies currently received, or required by the patient:
Does the patient require assistance with, or provision of, skilled tasks (e.g. monitoring of vital signs, dressing changes, glucose monitoring, etc.)?
Yes
No
If Yes, please indicate:
Based on the medical condition, do you recommend the provision of service to assist with skilled tasks, personal care and/or light housekeeping tasks?
Yes
No
Contributing Factors:
Describe contributing factors including but not limited to the social, family, home or medical (e.g. muscular/motor impairments, poor range of motion,
decreased stamina, etc.) situation that may affect the patient’s ability to function, or may affect the need for home care or that may affect the patient's need
for assistance with skilled tasks, personal care tasks and/or light housekeeping. Please include any other information that may be pertinent to the need for
assistance with home care services.
IT IS MY OPINION THAT THIS PATIENT CAN BE CARED FOR AT HOME. I HAVE ACCURATELY DESCRIBED HIS OR HER MEDICAL CONDITION. NEEDS AND REGIMENS, INCLUDING ANY MEDICATION REGIMENS, AT THE TIME I EXAMINED HIM OR HER. I UNDERSTAND THAT I AM NOT TO RECOMMEND THE NUMBER OF HOURS OF PERSONAL CARE SERVICES THIS PATIENT MAY REQUIRE. I ALSO UNDERSTAND THAT THIS PHYSI- CIAN'S ORDER IS SUBJECT TO THE NEW YORK STATE DEPARTMENT OF HEALTH REGULATIONS AT PARTS 515, 516, 517 AND 518 OF TITLE 18 NYCRR, WHICH PERMIT THE DEPARTMENT TO IMPOSE MONETARY PENALTIES ON, OR SANCTION AND RECOVER OVERPAYMENTS FROM, PROVIDERS OR PRESCRIBERS OF MEDICAL CARE, SERVICES OR SUPPLIES WHEN MEDICAL CARE, SERVICES OR SUPPLIES THAT ARE UNNECESSARY, IMPROPER OR EXCEED THE PATIENT’S DOCUMENTED MEDICAL CONDITION ARE PROVIDED OR ORDERED.
INCOMPLETE OR MISSING INFORMATION MAY DELAY SERVICES TO THIS PATIENT
Physician’s Signature _________________________________________________________________ Date _________________________
PLEASE SIGN AND RETURN COMPLETED FORM WITHIN 30 CALENDAR DAYS OF EXAMINATION TO:
___________________________________________________________________________
___________________________________________________________________________
___________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
__________________________________________________________________________
New York State Department of Health
- 2 -
PHYSICIAN’S ORDER FOR PERSONAL CARE/CONSUMER DIRECTED PERSONAL ASSISTANCE SERVICES
INSTRUCTIONS
COMPLETE ALL ITEMS. (Attach additional sheets, if necessary). INCOMPLETE FORMS WILL BE RETURNED TO THE PHYSICIAN.
INCOMPLETE OR MISSING INFORMATION MAY DELAY SERVICES TO THIS PATIENT.
1.Patient Identifying Information
•Patient Name. Enter the patient’s name.
•CIN. Found on the patient’s Medical Assistance ID card.
•Date of Birth. Enter the patient’s date of birth.
•Sex. Enter the patient’s gender.
•Address and telephone number. Enter the patient’s address and telephone number.
•Medicare #. Enter the patient’s Medicare number if available.
•If currently hospitalized. If the patient is hospitalized at the time of completion of the physician's order, indicate the name of the hospital, date of admission, and anticipated date of discharge.
•Discharge to above address. If the patient is to be discharged to an address other than the address listed above please explain.
•General Information
Physician’s Name, License #, Address, Telephone. Enter information for the physician signing the order. Enter either the physician’s license number as issued by the New York State Department of Education or the provider billing number issued by the New York State Department of Health Medicaid Management Information System.
•Examination conducted by other than a physician. If patient was examined, and the order form completed by a physician’s assistant, specialist’s assistant, or nurse practitioner, complete the required information.
•Place of Examination. Indicate the location (office, clinic, home, etc) of the examination of the patient.
•Date of Examination. Enter the date the patient was examined. This must be within 30 days of the date the physician signed the form.
3.Medical Findings
Note: Indicate N/A if an item does not apply to this patient or Unk if the requested information is unknown to the physician signing this form.
•Height, Weight. Enter the patient’s height and weight.
•Primary and Secondary Diagnosis. Enter the primary and secondary diagnosis with
•Describes the current condition. Describe the patient’s current medical/physical condition, including any relevant history.
•Stability. Check Yes if the patient’s condition is not expected to show marked deterioration or improvement. A stable medical condition shall be defined as follows:
(a)the condition is not expected to exhibit sudden deterioration or improvement; and
(b)the condition does not require frequent medical or nursing judgment to determine changes in the patient's plan of care; and
(c)(1) the condition is such that a physically disabled individual is in need of routine supportive assistance and does not need skilled professional care in the home; or
(2)the condition is such that a physically disabled or frail elderly individual does not need professional care but does require assistance in the home to prevent a health or safety crisis from developing.
•Hospice. If the patient’s condition is terminal, indicate if the patient is appropriate for Hospice services.
•Describe the current treatment plan. Include therapeutic goals and prognosis for recovery and anticipated duration of the current treatment plan.
•Limitations. Indicate any functional limitations or prohibited activities.
•
•Able to Summon Help. Check Yes if the patient is able to summon assistance in an emergency situation by any means. If the patient is not able to summon assistance, check No and explain.
-3 -
•Ambulation. Indicate the patient’s ability to ambulate independently, or with the need for assistance or devices. Specify assistance/devices used or needed.
•Bowel/Bladder. Indicate if the patient is continent. Describe any catheter or colostomy needs.
•Medications Required. List all prescription and
•Medication Administration. Indicate the patient’s ability to
•Dietary Needs. Indicate if the patient has special nutritional or dietary needs, i.e. low salt or high potassium.
•Tasks/Treatments/Therapies. Indicate any tasks, treatments or therapies which the patient receives or requires in the home and describe.
•Need for completion/assistance with skilled tasks. If the patient requires assistance with skilled tasks including, but not limited to, glucose monitoring, wound care, vital signs, describe the need for such assistance.
•Recommendation to provide assistance. Check Yes if, in your opinion, the patient can be maintained in his or her home with provision of home care services.
•Contributing factors to need for assistance. Please indicate the functional deficits that support the need for the provision of home care services. Please include any pertinent information you may have regarding the patient’s surroundings, physical condition or other factors that may affect the ability of the patient to function in the community or the patient’s need for assistance with personal care tasks.
4.Physician’s Signature/Date of completion. The signature of the ordering physician as identified in Item 2. Note that by signing this document, the physician certifies that the patient’s condition and needs are accurately described. Forms lacking a signature and/or date are not acceptable.
5.Return Form To. The local district or other case management entity to whom the form is to be returned.
- 4 -
| Fact Name | Description |
|---|---|
| Form Title | DOH-4359 is titled "Physician’s Order for Personal Care/Consumer Directed Personal Assistance Services". |
| Year of Release | This form was released in 2010, reflecting the standards and requirements of that period. |
| Patient Information | The form gathers essential details such as the patient's name, date of birth, address, and Medicare number. |
| Physician Details | It requires information from the physician including their name, license number, and the location where the examination took place. |
| Medical Findings | Physicians must document specific medical information, including primary and secondary diagnoses and the patient's condition. |
| Signature Requirement | The physician's signature and date are mandatory for the form to be considered valid and acceptable. |
| State Regulations | The form is governed by New York State Department of Health regulations under Title 18 NYCRR, specifically Sections 515-518. |
| Submission Deadline | The completed form must be submitted within 30 calendar days of the examination to avoid delays in services. |
Completing the DOH-4359 form is crucial in ensuring that the necessary personal care services are authorized for the patient. Follow these steps carefully to fill out the form accurately.
What is the DOH 4359 form?
The DOH 4359 form is a Physician’s Order for Personal Care Services or Consumer Directed Personal Assistance Services. It is used to document a patient’s medical condition, needs for care at home, and to request assistance services. Accurate completion is essential to ensure that patients receive the necessary support without undue delays.
Who is required to complete the DOH 4359 form?
The form must be completed by a licensed physician. If an examination is conducted by a physician’s assistant, specialist's assistant, or nurse practitioner, their information must also be included on the form. The physician must ensure that all items are filled out accurately and completely.
What information must be included on the form?
Critical information includes the patient’s identifying information, details about the physician, and medical findings. This includes the patient’s height, weight, diagnoses with ICD-9-CM codes, treatment plan, medication needs, and functional limitations. Missing or incomplete information can lead to delays in service.
Why is it important to fill out every item on the DOH 4359 form?
Every item on the form is designed to gather specific information that supports the patient's eligibility for services. Incomplete forms will be returned to the physician, which may delay the provision of necessary care. Thorough completion ensures the patient is assessed correctly and receives appropriate help.
How does the physician certify the information on the form?
By signing the DOH 4359 form, the physician certifies that the medical condition and needs of the patient are accurately documented. This signature is a vital part of the process. Forms without a physician’s signature or date are not considered valid.
What happens if the patient is currently hospitalized?
If the patient is hospitalized, the physician must provide the name of the hospital, date of admission, and the anticipated date of discharge. This information is crucial for coordinating the patient’s care upon discharge and ensuring continuity of services once they return home.
What are contributing factors in the context of the DOH 4359 form?
Contributing factors refer to any social, family, or medical circumstances that affect the patient's ability to function. This includes physical impairments, environmental challenges, or lack of support systems at home. These factors are essential in determining the patient's need for assistance with personal care tasks or skilled care.
Is there a time limit for submitting the DOH 4359 form?
Yes, the completed form must be returned within 30 calendar days from the date of the examination. Timeliness is important to avoid delays in the initiation of services. An expired form may not be accepted, leading to further complications for the patient.
What should a physician do if an item does not apply to the patient?
In instances where a particular item does not apply, the physician should indicate "N/A" for that item. If the requested information is unknown, the physician should write "Unk." This clarity is necessary for proper evaluation and ensures that all relevant sections of the form are addressed.
What kinds of services can be requested through the DOH 4359 form?
The form can be used to request a variety of home care services, including personal care assistance and consumer-directed personal assistance services. This may also involve skilled tasks such as monitoring vital signs or administering medications, depending on the needs of the patient.
Failing to Complete All Items: Many people leave sections blank. Every part of the Doh 4359 form must be filled out. Incomplete forms will be returned, delaying the process for the patient.
Incorrect Patient Identifying Information: Mistakes in the patient's name, date of birth, or address can cause significant issues. Always double-check this information to ensure accuracy.
Inaccurate Medical Findings: Providing incorrect diagnoses or entering wrong ICD-9-CM codes leads to complications. It’s crucial to list the patient's medical conditions correctly.
Neglecting Signature and Date: Forgetting to sign or date the form renders it invalid. The physician's signature is mandatory to confirm that the information is correct.
Not Describing Limitations Clearly: Ambiguous or vague descriptions of the patient’s functional limitations can mislead reviewers. Ensure all limitations and needs are clearly detailed.
The DOH-4359 form, titled "Physician’s Order for Personal Care/Consumer Directed Personal Assistance Services," is crucial for determining a patient's eligibility for home care services. Along with this form, several other documents are often required. Each serves a unique purpose to ensure the patient's needs are accurately assessed and appropriately met.
Having these documents prepared and properly completed can significantly streamline the process for patients and caregivers. It can ultimately contribute to more effective care and support for those in need.
The DOH-4359 form, known as the Physician’s Order for Personal Care/Consumer Directed Personal Assistance Services, has similarities with the Medical Necessity Certificate (MNC). The MNC is a form that confirms a patient's need for specific medical equipment, treatments, or services. Both documents require detailed patient information, including demographics and medical conditions, to justify the necessity of care or assistance. Just as the DOH-4359 provides a snapshot of the patient's health status and required services, the MNC outlines the medical rationale behind the necessity of specific interventions, ensuring that the patient's health plan is appropriately aligned with their needs.
Another document comparable to the DOH-4359 is the Home Health Care Plan. This plan outlines the type of medical and personal care a patient will receive at home. Like the DOH-4359, it includes assessments of the patient's medical condition, current abilities, and the type of services required for their care. Each document emphasizes individualized care tailored to the patient's specific needs. Furthermore, both documents require signatures from healthcare providers to validate the information and confirm the appropriateness of the care outlined.
The Durable Medical Equipment (DME) Prescription form also draws parallels to the DOH-4359. This form serves to prescribe and authorize medical equipment necessary for a patient's care. Similar to the DOH-4359, it requires identification of the patient, an explanation of the medical condition, and recommendations for specific services or equipment. Both forms involve a collaborative approach among healthcare providers to ensure a comprehensive plan that addresses the patient's needs and well-being.
Finally, the Personal Care Service Plan (PCSP) is akin to the DOH-4359 in terms of its focus on personal assistance needs. The PCSP is used to detail the non-medical support required for individuals, including activities of daily living. It reflects the patient's overall condition, current capabilities, and any limitations they face. Both the PCSP and the DOH-4359 emphasize the importance of tailoring assistance to fit the patient's unique circumstances, thus ensuring personalized care is delivered effectively.
When it comes to filling out the DOH-4359 form, careful attention is vital. Following these guidelines can help ensure accurate and timely processing.
By keeping these points in mind, you can help facilitate a smoother experience for both the patient and the healthcare providers involved.
Some believe that submitting an incomplete form will not affect the processing of requests. In reality, any missing or inaccurate information will result in the form being returned to the physician.
This is incorrect. Physicians must provide a detailed description of the patient’s condition and needs, but they should not recommend specific hours of personal care services on the form.
The DOH 4359 is applicable to any patient who may require personal care services, regardless of whether they are currently receiving such care at home or are in a hospital setting.
This view is misleading. While the form initiates the request for services, further communication or documentation may be necessary to ensure timely processing and approval.
This is not true. The DOH 4359 explicitly requests information regarding social, family, and environmental factors that may impact a patient's ability to function, highlighting the holistic approach to home care assessments.
The DOH-4359 form is essential for requesting personal care and Consumer Directed Personal Assistance Services (CDPAS) for patients.
Accurate patient identifying information is crucial. Ensure every section, including name, address, and date of birth, is thoroughly filled out.
The form requires a physician's signature. This confirms the accuracy of the information regarding the patient’s condition and needs.
Incomplete forms will be returned. Always double-check for missing information to avoid delays in service.
Medical findings section must include detailed descriptions of the patient’s conditions. Specify primary and secondary diagnoses using ICD-9-CM codes.
Note whether the patient’s condition is stable. A stable condition generally does not require frequent medical assessments.
Provide information about medication, including prescribed and over-the-counter drugs. This helps ensure the patient receives appropriate care.
Document any dietary needs. Indicate if the patient requires a modified diet or has specific nutritional requirements.
Be specific about the patient's need for assistance. Detail whether the patient requires help with medication administration or skilled tasks.
Return the completed form within 30 calendar days of the examination to the designated local district or case management entity.