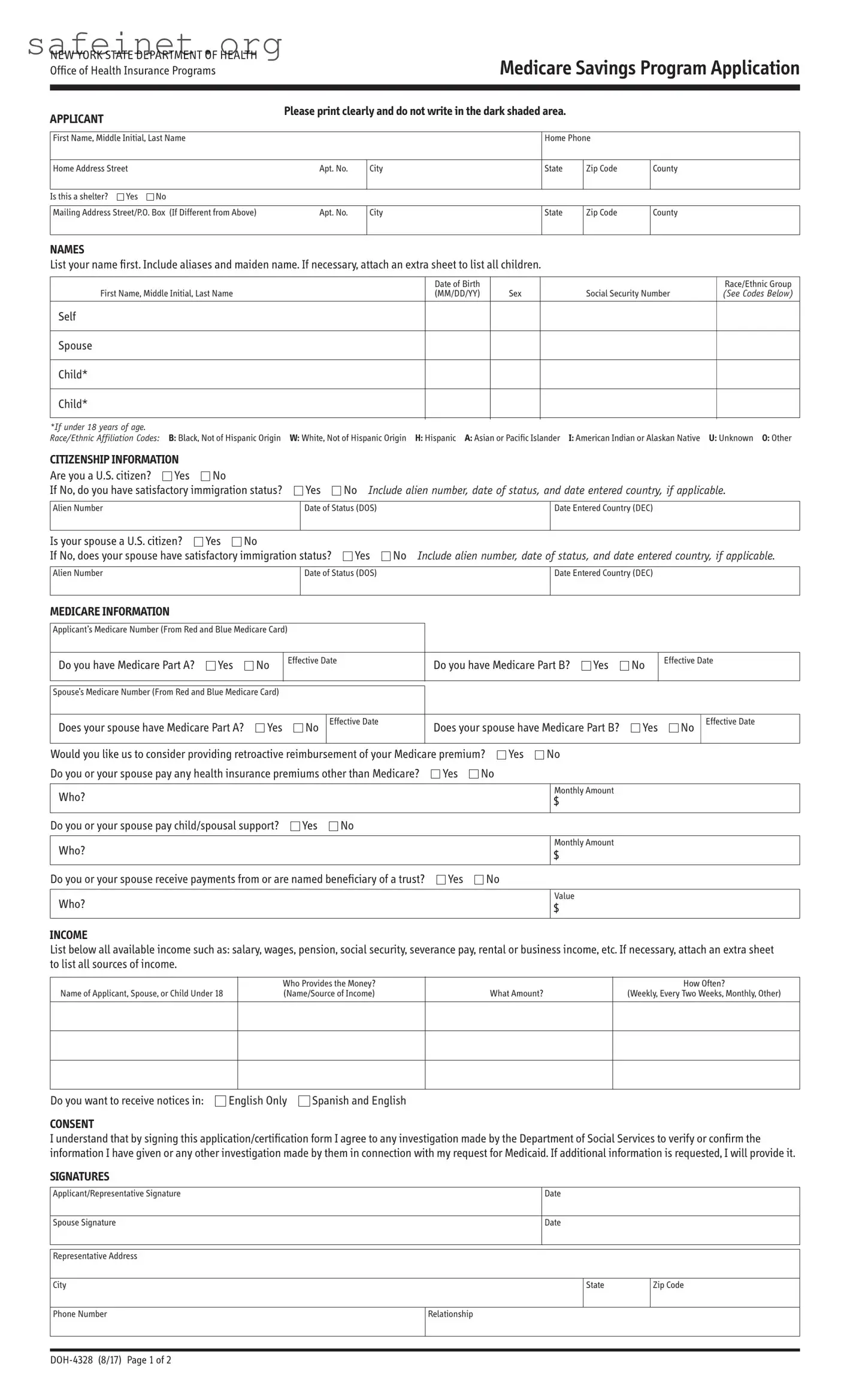
The DOH 4328 MSP Application form is a crucial document for individuals seeking to enroll in the Medicare Savings Program (MSP) through the New York State Department of Health. This program is designed to assist those with limited income in paying their Medicare premiums, ultimately making healthcare more accessible. The form requires applicants to provide essential information, including personal identification details such as names and Social Security numbers, as well as citizenship status and Medicare information. Income disclosures are central to the application, where applicants must list all sources of income, ensuring that each source is accurately documented. If applicable, the form also allows for details about dependents to be included. Clear instructions guide applicants through the verification process, emphasizing the importance of documentation, such as proof of income and residency. Additionally, by signing the application, individuals consent to investigations that may verify the provided information, underscoring both the seriousness and the importance of honesty in the process. This comprehensive approach ensures that the program effectively serves those in need while adhering to state and federal regulations.
NEW YORK STATE DEPARTMENT OF HEALTH Office of Health Insurance Programs
Medicare Savings Program Application
APPLICANT |
|
|
Please print clearly and do not write in the dark shaded area. |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
First Name, Middle Initial, Last Name |
|
|
Home Phone |
|
|||
|
|
|
|
|
|
|
|
Home Address Street |
|
Apt. No. |
City |
State |
Zip Code |
County |
|
|
|
|
|
|
|
|
|
Is this a shelter? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
||
Mailing Address Street/P.O. Box (If Different from Above) |
Apt. No. |
City |
State |
Zip Code |
County |
||
|
|
|
|
|
|
|
|
NAMES
List your name first. Include aliases and maiden name. If necessary, attach an extra sheet to list all children.
|
Date of Birth |
|
|
Race/Ethnic Group |
First Name, Middle Initial, Last Name |
(MM/DD/YY) |
Sex |
Social Security Number |
(See Codes Below) |
Self
Spouse
Child*
Child*
*If under 18 years of age.
Race/Ethnic Affiliation Codes: B: Black, Not of Hispanic Origin W: White, Not of Hispanic Origin H: Hispanic A: Asian or Pacific Islander I: American Indian or Alaskan Native U: Unknown O: Other
CITIZENSHIP INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Are you a U.S. citizen? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If No, do you have satisfactory immigration status? |
|
|
|
Yes |
No Include alien number, date of status, and date entered country, if applicable. |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Alien Number |
|
|
|
|
|
|
|
|
|
|
Date of Status (DOS) |
|
|
|
|
|
Date Entered Country (DEC) |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Is your spouse a U.S. citizen? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
If No, does your spouse have satisfactory immigration status? |
Yes |
No Include alien number, date of status, and date entered country, if applicable. |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Alien Number |
|
|
|
|
|
|
|
|
|
|
Date of Status (DOS) |
|
|
|
|
|
Date Entered Country (DEC) |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICARE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Applicant’s Medicare Number (From Red and Blue Medicare Card) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Do you have Medicare Part A? |
|
Yes |
|
|
No |
Effective Date |
|
|
Do you have Medicare Part B? |
|
Yes |
|
|
No |
Effective Date |
||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Spouse’s Medicare Number (From Red and Blue Medicare Card) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Does your spouse have Medicare Part A? |
|
Yes |
|
|
|
No Effective Date |
|
Does your spouse have Medicare Part B? |
|
Yes |
|
|
No Effective Date |
||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Would you like us to consider providing retroactive reimbursement of your Medicare premium? |
Yes |
No |
|
|
|
|
|
|
|
|
|
||||||||||||||||
Do you or your spouse pay any health insurance premiums other than Medicare? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Who? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Monthly Amount |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Do you or your spouse pay child/spousal support? |
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Who?
Monthly Amount
$
Do you or your spouse receive payments from or are named beneficiary of a trust? |
Yes |
No |
Who?
Value
$
INCOME
List below all available income such as: salary, wages, pension, social security, severance pay, rental or business income, etc. If necessary, attach an extra sheet to list all sources of income.
Name of Applicant, Spouse, or Child Under 18
Who Provides the Money? (Name/Source of Income)
What Amount?
How Often?
(Weekly, Every Two Weeks, Monthly, Other)
Do you want to receive notices in:
English Only
Spanish and English
CONSENT
I understand that by signing this application/certification form I agree to any investigation made by the Department of Social Services to verify or confirm the information I have given or any other investigation made by them in connection with my request for Medicaid. If additional information is requested, I will provide it.
SIGNATURES
Applicant/Representative Signature |
|
Date |
|
|
|
|
|
|
|
Spouse Signature |
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
Representative Address |
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip Code |
|
|
|
|
|
Phone Number |
Relationship |
|
||
|
|
|
|
|
|
|
|
|
|
INSTRUCTIONS
COMPLETE THE APPLICATION
Be sure to answer all the questions. If you are married and living with your spouse, you must complete both the “Self” and “Spouse” questions on the application (even if the spouse is not applying for the MSP).
SIGN AND DATE THE APPLICATION
If both spouses are applying, both must sign the MSP application.
INCLUDE THE FOLLOWING VERIFICATION DOCUMENTS
Please review this list and submit the documents that you will need to provide in order for the Medicaid Program to determine if you are eligible for MSP. If you are requesting retroactive reimbursement of your Medicare premiums, you must send proof of income for the previous
•A photocopy of the front and back of your Medicare card.
•Proof of income: Paycheck stubs, letter from employer, income tax return, award letter for any unearned income benefit such as social security, unemployment, or veteran’s benefit, or letter from renter, boarder or tenant.
•Health insurance premiums that you pay other than Medicare: Letter from employer, premium statement, or pay stub.
•Proof of date of birth: State driver’s license, U.S. birth certificate, permanent resident card (“green card”), or NYS Benefit Identification Card.
•Proof of residence: Lease/letter/rent receipt with your home address from your landlord, driver’s license (if issued in the past 6 months), utility bill (gas, electric, phone, cable, fuel or water), government ID card with address, property tax records or mortgage statement, or postmarked envelope or postcard (cannot use if sent to a P.O. Box).
•If you are not a U.S. citizen, you must provide documents indicating your current immigration status.
Mail the application and required documentation to your local Department of Social Services (LDSS) or Human Resource Administration (HRA). To find the address in your county: http://www.health.ny.gov/health_care/medicaid/ldss.htm
TERMS, RIGHTS AND RESPONSIBILITIES
By completing and signing this form, I am applying for the Medicare Savings Program. PAYMENT OF YOUR MEDICARE PREMIUM IS A MEDICAID BENEFIT.
PENALTIES
I understand that my application may be investigated, and I agree to cooperate in such an investigation. Federal and State laws provide for penalties of fine, imprisonment or both if you do not tell the truth when you apply for Medicaid benefits or at any time when you are questioned about your eligibility, or cause someone else not to tell the truth regarding your application or your continuing eligibility.
CHANGES
I agree to immediately report any changes to the information on this application.
SOCIAL SECURITY NUMBER (SSN)
If you are applying for the Medicare Savings Program, you must report your SSN, unless you are a pregnant woman. The laws requiring this are: 18NYCRR Sections 351.2,
CERTIFICATION OF CITIZENSHIP & IMMIGRATION STATUS
I certify, under the penalty of perjury, by signing my name on this application, that I, and/or any person for whom I am signing is a U.S. citizen or national of the United States or has satisfactory immigration status. I understand that information about me will be submitted to the United States Citizenship and Immigration Services (USCIS) for verification of my immigration status, if applicable. I further understand that the use or disclosure of information about me is restricted to persons and organizations directly connected with the verification of immigration status and the administration and enforcement of the provisions of the Medicaid program.
This application will be considered without regard to race, color, sex, disability, religious creed, national origin, or political belief.
CERTIFICATION
In signing this application, I swear and affirm that the information I have given or will give to the Department of Social Services as a basis for Medicaid is correct. I also assign to the Department of Social Services any rights I have to pursue support from persons having legal responsibility for my support and to pursue other
If after reading and completing this form, you decide that you DO NOT want to apply for the Medicare Savings Program, please sign your name below:
I consent to withdraw my application:
Applicant Signature
Date
Signature of Person Who Obtained Eligibility Information |
|
|
Date |
Employed By |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Date Eligibility Determined By Worker |
|
|
|
|
|
Date Eligibility Approved By |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Central/Office |
Application Date |
|
Unit ID |
|
Worker ID |
Case Type |
Case No. |
|
|
Reuse Ind. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Case Name |
|
|
District |
|
|
|
Registry No. |
|
Ver. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Effective Date |
|
MA Disp. |
Denial |
Withdrawal |
Reason Code |
|
Proxy |
No |
|||
|
|
|
|
Yes |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
| Fact Name | Details |
|---|---|
| Applicant Identification | The form requires the applicant's full name, home address, and phone number for identification purposes. |
| Citizenship Status | Applicants must affirm their U.S. citizenship status and provide details if they are not citizens. |
| Medicare Information | Applicants must list their Medicare numbers and provide information on Medicare Part A and B status. |
| Income Reporting | Applicants are required to list all sources of income to determine eligibility for the Medicare Savings Program. |
| Verification Documents | Submission of specific documents, such as Medicare cards and proof of income, is essential for application processing. |
| Consents and Agreements | Signing the application grants the Department of Social Services permission to verify provided information. |
| Non-Discrimination Notice | The application is processed without regard to race, color, or other protected characteristics. |
| Reporting Changes | Applicants must immediately report any changes affecting their application after submission. |
| Applicable State Laws | This form is governed by New York State regulations including 18 NYCRR Sections 351.2, 360-1.2, and 360-3.2(j)(3). |
Completing the Doh 4328 MSP Application form is essential for individuals seeking assistance under the Medicare Savings Program. Ensuring accuracy and completeness in this process is crucial to facilitate a smoother review of your application. You will need to carefully gather personal information, income details, and supporting documents before submitting the application to your local Department of Social Services.
What is the DOH 4328 MSP Application form used for?
The DOH 4328 MSP Application form is used to apply for the Medicare Savings Program (MSP) in New York State. This program helps eligible individuals pay for some or all of their Medicare premiums, which can alleviate financial strain on seniors and those with disabilities.
Who is eligible to apply for the Medicare Savings Program?
To be eligible for the MSP, applicants must be Medicare beneficiaries and meet specific income and resource limits. Both individuals and married couples can apply. If you're unsure about your eligibility, consider reaching out to local social services for guidance.
What information do I need to provide on the application?
You must provide personal details, including your name, contact information, and Social Security Number. Additionally, you'll need to list your income and assets, Medicare information, and citizenship status. Documentation to verify this information may also be required.
How do I submit the DOH 4328 MSP Application form?
Once you complete the application and gather the necessary verification documents, mail it to your local Department of Social Services (LDSS) or Human Resource Administration (HRA). You can find the appropriate address for your county on the New York State Health Department website.
What happens if I need to make changes after submitting my application?
If any changes occur regarding your income or circumstances, report them immediately. Keeping your information updated ensures you maintain your eligibility and avoid issues with your benefits.
Is there a penalty for providing false information?
Yes. Providing false information on the application can result in penalties, including fines or imprisonment. It's crucial to give accurate and truthful information during the application process and whenever your eligibility is reviewed.
Inadequate Detail: Failing to provide complete information is a common mistake. Each section, such as personal details, income, and Medicare information, must be thoroughly filled out. Omitting details can lead to delays in processing.
Incorrect Signatures: Not signing or dating the application can result in rejection. Both the applicant and spouse, if applicable, must sign where indicated. A missing signature delays the application.
Using Dark Ink or Poor Readability: The instructions specify that the form should be printed clearly. Using dark or faded ink makes the writing hard to read, which can cause errors in data entry.
Inadequate Documentation: Many applicants do not include necessary verification documents. For eligibility, proof of income, identity, and citizenship must be attached. Insufficient documentation can lead to application denial.
The **DOH 4328 MSP Application Form** is a crucial document for those seeking assistance through the Medicare Savings Program in New York. However, several other forms and documents are often required to complete the application process and provide a full picture of an applicant's financial and personal situation. Below is a list of essential documents that may accompany the DOH 4328. Each plays a specific role in supporting the application.
These documents collectively provide necessary evidence for determining eligibility and ensuring smooth processing of the DOH 4328 MSP Application Form. It is critical to gather all required documentation before submission to avoid delays in the assistance process.
The DOH 4328 MSP Application form bears resemblance to the Social Security Administration's Application for Right to Work, known as Form I-765. Similar to the DOH 4328, this form requires personal information such as name, address, and Social Security number. Both forms also necessitate documentation to confirm identity and eligibility related to specific benefits. They aim to ensure applicants can access essential services by collecting a standard set of information needed for processing their requests.
Additionally, the Medicaid Application form shares characteristics with the DOH 4328. The Medicaid Application asks for detailed information regarding an applicant’s income, resources, and family structure, mirroring the income information collected on the Medicare Savings Program application. Both forms require documentation that verifies the information provided, ensuring that the applicant meets financial eligibility criteria for receiving benefits.
Another similar document is the Supplemental Nutrition Assistance Program (SNAP) application. The SNAP application, like the DOH 4328, gathers extensive personal and financial information. Both documents aim to gauge the applicant's eligibility for government assistance programs. The need for supporting documents demonstrates a shared process of verification necessary for effective program administration.
The Low-Income Home Energy Assistance Program (LIHEAP) application also exhibits similarities to the DOH 4328. Both forms prompt applicants to provide personal data, household composition, and financial details. By requiring comprehensive information about income and expenses, both applications aim to determine eligibility for assistance with essential living expenses, such as energy costs in the case of LIHEAP.
The Medicare Part D Extra Help application parallels the DOH 4328 in its function. This form requires applicants to disclose personal demographic information, including household income and assets. Just like the MSP application, the Extra Help application assesses whether individuals meet the financial requirements to reduce their prescription drug costs, again focusing on the concept of financial need.
Another related document is the Temporary Assistance for Needy Families (TANF) application. The TANF application seeks information about household members, income, and expenses, mirroring the need for detailed personal and financial disclosures in the DOH 4328. The objective of both applications is to determine eligibility for assistance aimed at relieving financial stress among low-income families.
The Health Insurance Marketplace application also shares structural similarities with the DOH 4328. It requires applicants to submit personal information and assess their income levels to determine eligibility for health coverage options. Both applications facilitate access to federal and state health-related benefits, highlighting the importance of providing accurate information for program enrollment and support.
The Earned Income Tax Credit (EITC) application process functions similarly, asking for significant personal and financial details to determine eligibility for the credit. Similarly to the DOH 4328, the EITC requires supporting documentation to establish the applicant's income level and family size, thereby ensuring that benefits are appropriately allocated.
The Veterans Affairs (VA) Benefits application reflects similar requirements to the DOH 4328 as well. Both forms gather comprehensive personal details and income information to assess eligibility for benefits. The VA ensures that veterans receive the necessary support by capturing data that validates their need for assistance, paralleling the approach utilized in the Medicare Savings Program.
Finally, the Child Health Plus application presents further similarities to the DOH 4328. This application requires personal information and household income details to establish eligibility for health insurance coverage for children. Both applications focus on ensuring access to essential health services, hence requiring detailed financial disclosures from the applicants to verify their eligibility for support.
When filling out the Doh 4328 MSP Application form, consider these important do's and don'ts:
Understanding the DOH 4328 MSP Application form is essential for those seeking assistance with Medicare premiums. However, several misconceptions can create confusion. Below are some common misunderstandings:
By clarifying these misconceptions, applicants can approach the DOH 4328 MSP Application with confidence and ensure they provide all necessary information for a successful application process.
Applying for the Medicare Savings Program using the DOH 4328 MSP Application form can be a vital step in managing healthcare costs. Here are four key takeaways to keep in mind when filling out and using the application: