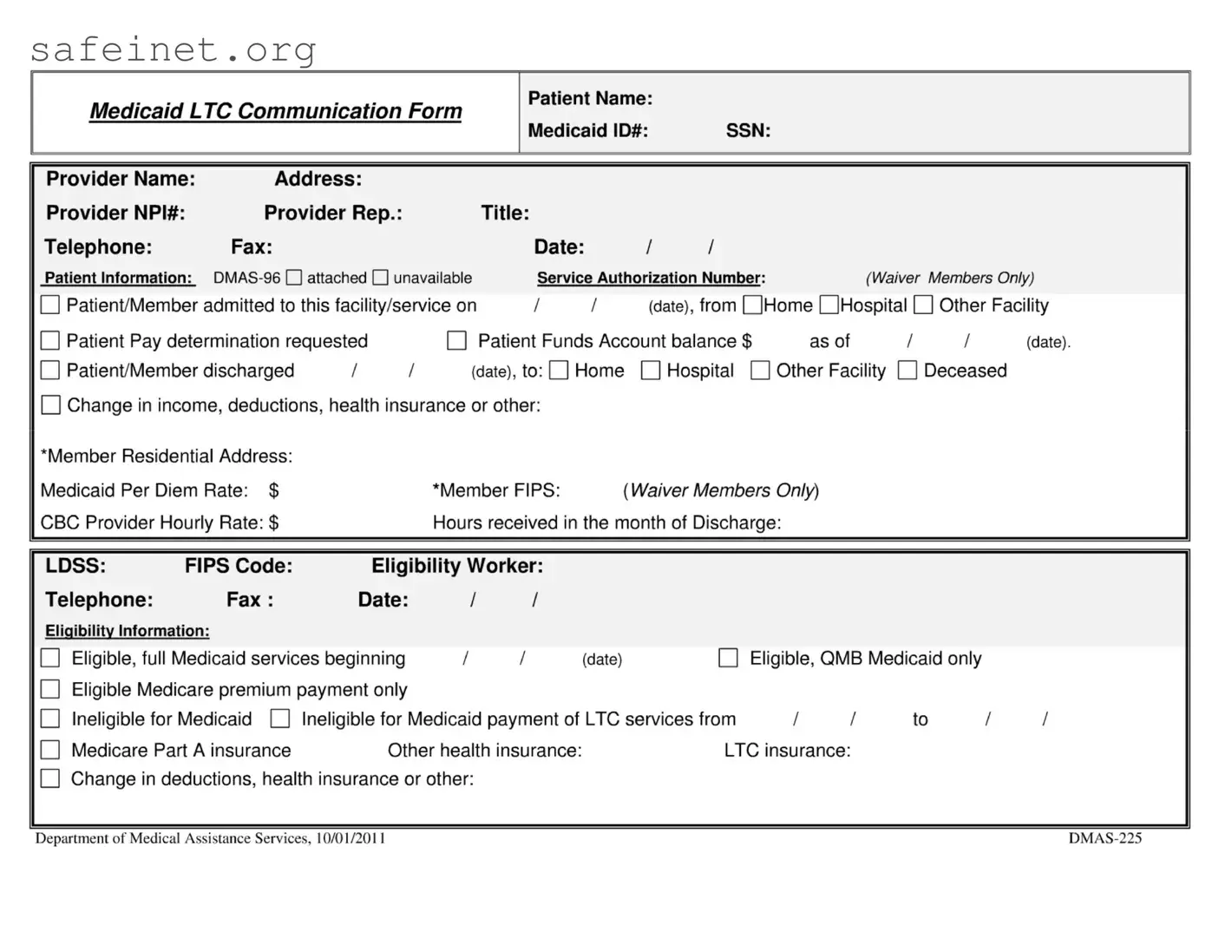
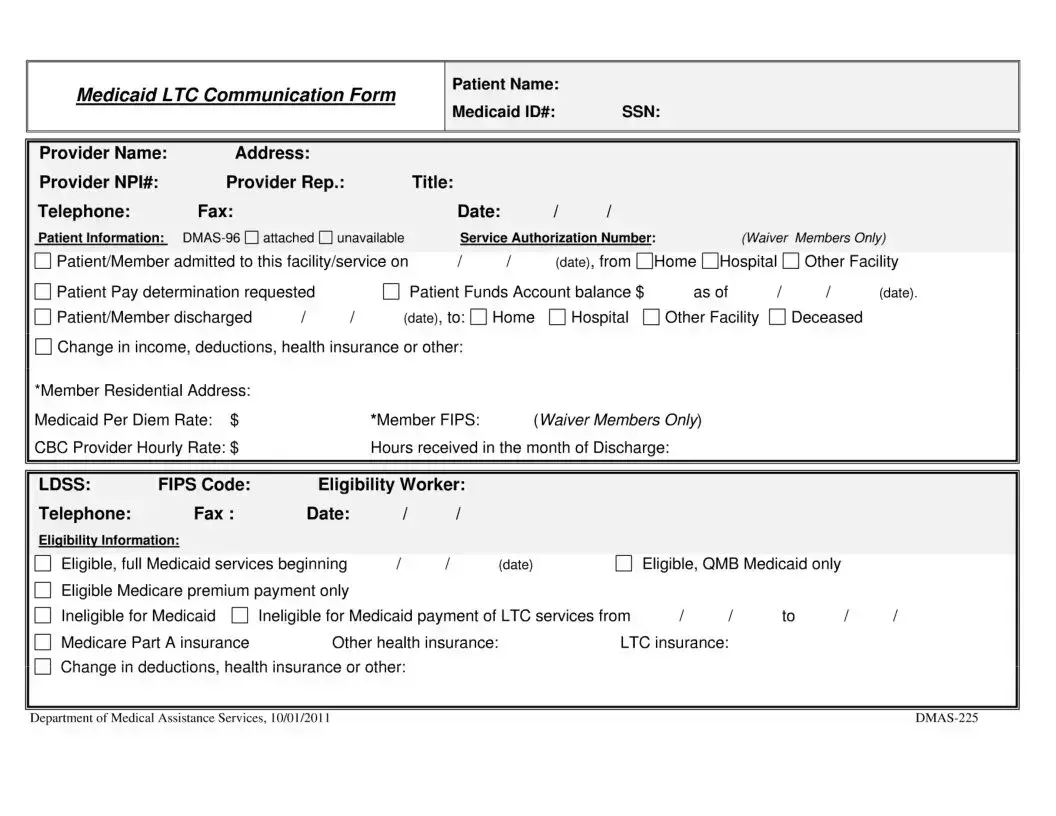
The DMAS 225 form plays a crucial role in facilitating communication between various healthcare providers, local departments of social services (LDSS), and Medicaid recipients in long-term care situations. This comprehensive form is designed to document essential details regarding a patient's Medicaid eligibility status, changes in their level of care, and significant events such as admissions, discharges, or even death. It also includes pertinent information about the patient's financial situation, including any patient pay determinations and available funds. Initiated by either the LDSS or the provider, the DMAS 225 ensures that all relevant parties remain informed about the patient's changing circumstances. The form must be completed accurately to convey necessary details to the appropriate individuals and agencies, promoting a collaborative approach to managing the patient's care and benefits. Copies of the form need to be distributed to specific entities, reinforcing communication and assisting in timely decision-making related to the patient's Medicaid services and other related needs.
Medicaid LTC Communication Form
Patient Name:
Medicaid ID#: |
SSN: |
Provider Name: |
Address: |
|
|
|
|
|
|
|
|
|
|
|
Provider NPI#: |
Provider Rep.: |
|
|
Title: |
|
|
|
|
|
|
|
|
Telephone: |
Fax: |
|
|
|
Date: |
/ |
/ |
|
|
|
|
|
Patient Information: |
|
Service Authorization Number: |
(Waiver Members Only) |
|||||||||
Patient/Member admitted to this facility/service on |
/ |
/ |
(date), from QHome OHospital |
|
Other Facility |
|||||||
Patient Pay determination requested |
|
|
Patient Funds Account balance $ |
as of |
I |
I |
(date). |
|||||
Patient/Member discharged |
/ |
/ |
(date), to: |
Home |
|
Hospital О Other Facility |
|
Deceased |
|
|||
Change in income, deductions, health insurance or other:
‘Member Residential Address:
Medicaid Per Diem Rate: $ |
‘Member FIPS: |
{WaiverMembers Only) |
CBC Provider Hourly Rate: $ |
Hours received in the month of Discharge: |
|
LDSS: FIPS Code: Eligibility Worker:
Telephone: |
Fax: |
Date: |
|
/ |
/ |
|
|
|
|
Eligibility Information: |
|
|
|
|
|
|
|
|
|
Eligible, full Medicaid services beginning |
1 |
/ |
(date) |
|
Eligible, QMB Medicaid only |
|
|||
Eligible Medicare premium payment only |
|
|
|
|
|
|
|
||
Ineligible for Medicaid |
Ineligible for Medicaid payment of LTC services from |
II |
to |
II |
|||||
Medicare Part A insurance |
Other health insurance: |
LTC insurance: |
|
|
|||||
Change in deductions, health insurance or other:
Department of Medical Assistance Services, 10/01/2011 |
Medicaid LTC Communication Form, Effective 10/01/2011 |
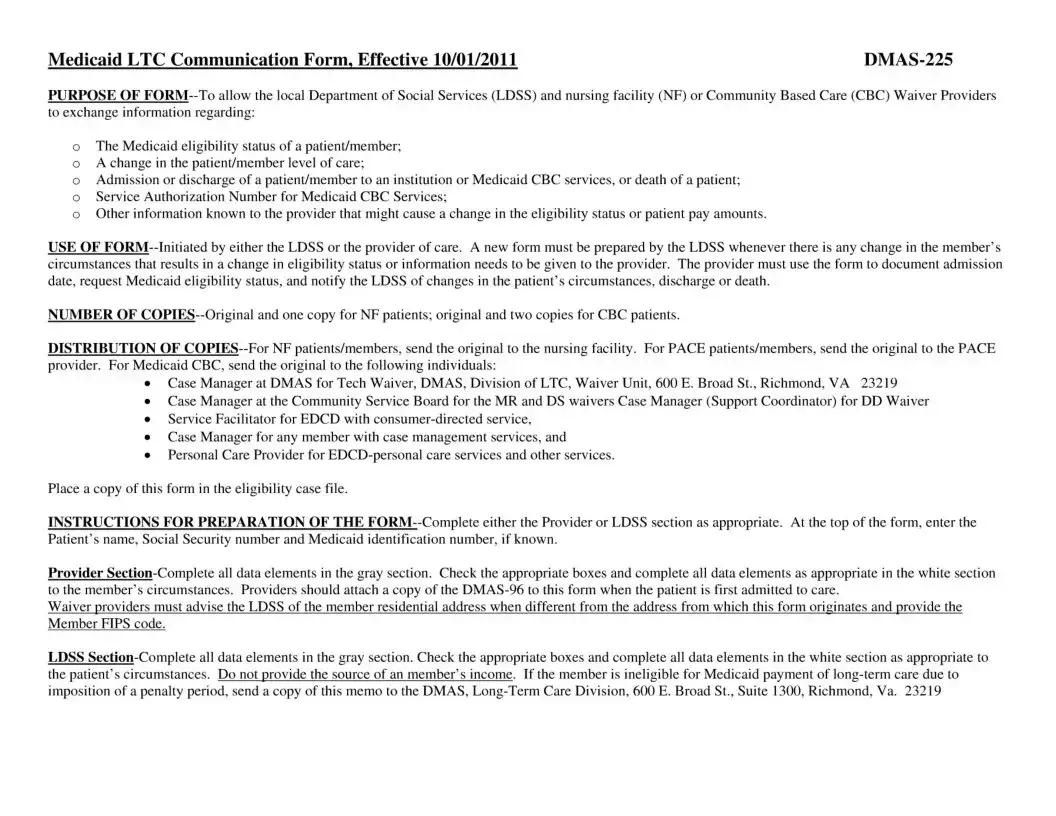
PURPOSE OF
оThe Medicaid eligibility status of a patient/member;
оA change in the patient/member level of care;
оAdmission or discharge of a patient/member to an institution or Medicaid CBC services, or death of a patient;
оService Authorization Number for Medicaid CBC Services;
оOther information known to the provider that might cause a change in the eligibility status or patient pay amounts.
USE OF
NUMBER OF
DISTRIBUTION OF
•Case Manager at DMAS for Tech Waiver, DMAS, Division of LTC, Waiver Unit, 600 E. Broad St., Richmond, VA 23219
•Case Manager at the Community Service Board for the MR and DS waivers Case Manager (Support Coordinator) for DD Waiver
•Service Facilitator for EDCD with
•Case Manager for any member with case management services, and
•Personal Care Provider for
Place a copy of this form in the eligibility case file.
INSTRUCTIONS FOR PREPARATION OF THE
Provider
Waiver providers must advise the LDSS of the member residential address when different from the address from which this form originates and provide the Member FIPS code.
LDSS
| Fact Name | Description |
|---|---|
| Purpose of Form | The DMAS 225 form is used to facilitate communication between the local Department of Social Services (LDSS) and care providers regarding a patient's Medicaid eligibility and care status. |
| Initiation of Form | Either the LDSS or the care provider can initiate the DMAS 225 form when there are changes in the patient's status or eligibility. |
| Required Copies | For nursing facility (NF) patients, the original and one copy are required. For Community-Based Care (CBC) patients, the original and two copies must be submitted. |
| Documentation Necessity | A new form must be prepared by the LDSS whenever there are changes to a member’s circumstances that affect eligibility or pay amounts. |
| Distribution Requirements | The original form must be sent to designated recipients such as the nursing facility, community service board, and case managers, depending on the type of patient. |
| Completion Sections | Sections of the form must be completed either by the provider or the LDSS, capturing all necessary information about the patient and their circumstances. |
| Attachments Needed | The provider must attach a copy of the DMAS-96 form to the DMAS 225 when the patient is first admitted to care. |
| Eligibility Information | The form requires detailed eligibility information, such as the patient’s Medicaid status, Medicare coverage, and any changes in income or health insurance. |
| Governing Law | This form is governed by guidelines from the Department of Medical Assistance Services (DMAS) effective 10/01/2011, pertaining to Medicaid long-term care. |
Once you have the DMAS 225 form ready, it’s important to fill it out accurately. This ensures proper communication between various health care providers and the Department of Medical Assistance Services concerning Medicaid patients. Follow these steps to complete the form effectively.
After filling out the DMAS 225 form, double-check all details for accuracy. Once confirmed, the next steps involve distributing copies as per the guidelines to relevant parties, ensuring seamless communication regarding the patient’s Medicaid status.
What is the purpose of the DMAS 225 form?
The DMAS 225 form is designed for communication between the local Department of Social Services (LDSS) and nursing facilities or Community Based Care (CBC) Waiver Providers. It allows both entities to share important information related to a patient or member’s Medicaid eligibility status, changes in their level of care, admission or discharge details, and any other significant updates that might affect their care or financial contributions.
Who should fill out the DMAS 225 form?
Either the local Department of Social Services or the provider of care can initiate the form. It’s crucial for the LDSS or the provider to complete the appropriate section based on their involvement with the patient. This ensures all relevant information is accurately conveyed between the parties involved in the patient’s care.
How many copies of the DMAS 225 form are required?
For patients at nursing facilities, you'll need to prepare the original form along with one copy. If the patient is enrolled in Community Based Care, prepare the original and two copies. Keeping the correct number of copies ensures that all necessary parties have the information they need without any delays.
When should a new DMAS 225 form be completed?
A new DMAS 225 form should be completed whenever there is a change in a member's circumstances that affects their eligibility status or care needs. This includes changes like admission to or discharge from a facility, updates regarding Medicaid eligibility, or changes in income or health insurance. Timely updates help ensure smooth communication and ongoing care.
What information do I need to include on the DMAS 225 form?
You’ll need to provide various details, including the patient's name, Social Security number, Medicaid ID, and eligibility information. For providers, specific sections such as admission dates, service authorization numbers, and any changes in the patient’s circumstances should be documented. Ensure all relevant sections are filled out accurately to facilitate effective communication.
How is the DMAS 225 form distributed?
The original DMAS 225 form must be sent to the appropriate facility or provider, depending on the patient’s status. For nursing facility patients, send the original to the nursing facility. For PACE or Community Based Care patients, distribute the form to various case managers and service facilitators involved in the patient's care. Keeping a copy in the eligibility case file is also important for record-keeping purposes.
What should I do if a member is ineligible for Medicaid?
If a member is found to be ineligible for Medicaid payment for long-term care due to a penalty period, it is crucial to inform the Long-Term Care Division of the Department of Medical Assistance Services. You'll need to send a copy of the notification to the appropriate address to ensure proper processing and avoid any future complications with care funding.
Incomplete Patient Information: Not filling in essential details such as the patient's name, Medicaid ID, or Social Security number leads to delays in processing the form.
Incorrect Dates: Entering the wrong admission or discharge dates can create confusion regarding the patient's status and eligibility.
Missing Supporting Documents: Failing to attach required documents like the DMAS-96 can result in the form being rejected or delayed.
Provider Section Errors: Not completing all fields in the Provider section, such as NPI number or provider’s contact information, hampers communication.
Confusing FIPS Codes: Providing incorrect or missing Member FIPS codes, particularly for Waiver members, can complicate eligibility verification.
Wrong Eligibility Status: Misreporting the eligibility status of the patient can lead to improper funding and care arrangements.
Failure to Report Changes: Not informing the LDSS of changes in the patient's income, deductions, or health insurance can impact their eligibility.
Inadequate Copy Distribution: Not distributing the required number of copies to the appropriate parties, such as nursing facilities or case managers, leads to communication gaps.
Ignoring Instructions: Overlooking the preparation instructions, particularly about which sections to complete, results in incomplete submissions.
Omitting Signatures: Forgetting to sign the form at submission can delay processing and acknowledgment of the patient's care needs.
The DMAS 225 Form is a critical document used in the context of Medicaid long-term care communications. Often, it is accompanied by other important forms and documents that serve various purposes in the healthcare and Medicaid systems. Below is a list of some of these related documents, which facilitate communication between providers, patients, and government agencies.
These forms and documents work together with the DMAS 225 Form to manage the complex requirements of Medicaid long-term care. Ensuring that each form is properly filled out and submitted can significantly influence the smooth processing of Medicaid services and the overall care experience for patients.
The DMAS-96 form closely mirrors the DMAS-225 in its role of documenting Medicaid eligibility and changes in patient circumstances. Like the DMAS-225, the DMAS-96 is also used by nursing facilities and the local Department of Social Services (LDSS) to communicate essential information about a member's eligibility status. The form requires detailed patient information and must be updated whenever there are changes, ensuring accurate and timely management of Medicaid services.
The CMS 1500 form serves a similar purpose in the healthcare domain by facilitating the billing process for medical services under Medicare and Medicaid. It collects information about the patient, the provider, and the services rendered, much like the DMAS-225 collects comparable data for long-term care services. While the DMAS-225 focuses specifically on institutional and community-based care, the CMS 1500 form is broader in scope, allowing providers to bill for individual medical services in a standardized format.
The 572 form (Medicaid Long-Term Care Provider Collaboration) is another related document that aids the exchange of critical information between healthcare providers and the Medicaid agency. Both the DMAS-225 and the 572 are essential in establishing and maintaining a patient’s eligibility for benefits. The 572 form dives deeper into the financial aspects of care, including the patient’s pay determination, thereby complementing the DMAS-225, which captures the timeline of care and eligibility changes.
Similar to the DMAS-225, the Notice of Action (NoA) document informs members of significant changes in their Medicaid benefits or eligibility. The NoA serves as an official communication tool to alert individuals about changes, providing justification and recourse options. Both documents aim to ensure clear communication between the Medicaid agency and the individual, maintaining transparency in the services provided.
Lastly, the Form SSA-827, Authorization to Disclose Information to the Social Security Administration, bears resemblance to the DMAS-225 through its requirement for clear consent and information sharing regarding a patient’s benefits and eligibility. This form allows for sharing vital information necessary to determine eligibility for various social safety net programs. Just as the DMAS-225 seeks to update and communicate patient information among providers, the SSA-827 ensures the appropriate entities can access the necessary data for evaluations and decisions regarding Medicare and Social Security benefits.
When filling out the DMAS 225 form, keep these guidelines in mind:
1. The DMAS-225 form is only for nursing facilities. This form is applicable to both nursing facilities and Community Based Care (CBC) Waiver Providers, allowing them to share essential information about a patient/member's Medicaid eligibility.
2. Once submitted, the DMAS-225 form does not need to be updated. The form must be updated whenever there is a change in the patient/member's circumstances. This includes changes in eligibility status, admission, discharge, or death.
3. The form is only needed for Medicaid recipients. While it primarily focuses on Medicaid patients, it also assists in managing information for members involved in Medicare and other health insurance programs.
4. Only the provider can submit the DMAS-225 form. The form can be initiated by either the local Department of Social Services (LDSS) or the care provider, highlighting its collaborative role in patient management.
5. Patients need to fill out the DMAS-225 form themselves. Completing the DMAS-225 form is the responsibility of the LDSS or the care provider. Patients do not need to fill it out.
6. One copy of the form is sufficient for all cases. Different requirements exist based on the type of care. For instance, nursing facility patients require the original and one copy, while CBC patients need the original and two copies.
7. Only eligibility information is included on the DMAS-225 form. Besides eligibility status, the form collects information on changes in the patient's level of care, service authorization, and any relevant information regarding the patient's circumstances.
8. The DMAS-225 form is the same for all states. This form is specific to Virginia and may differ from forms used in other states, reflecting local regulations and procedures.
9. Once the form is filled out, it's only sent to one party. The completed DMAS-225 form must be distributed to multiple parties, including the nursing facility, case managers, and personal care providers, ensuring everyone involved is informed.
10. The information on the DMAS-225 form is confidential and cannot be shared. While the form does contain sensitive information, sharing it among authorized entities is essential for effective care coordination and ensuring proper service delivery.
Key Takeaways for Using the DMAS 225 Form