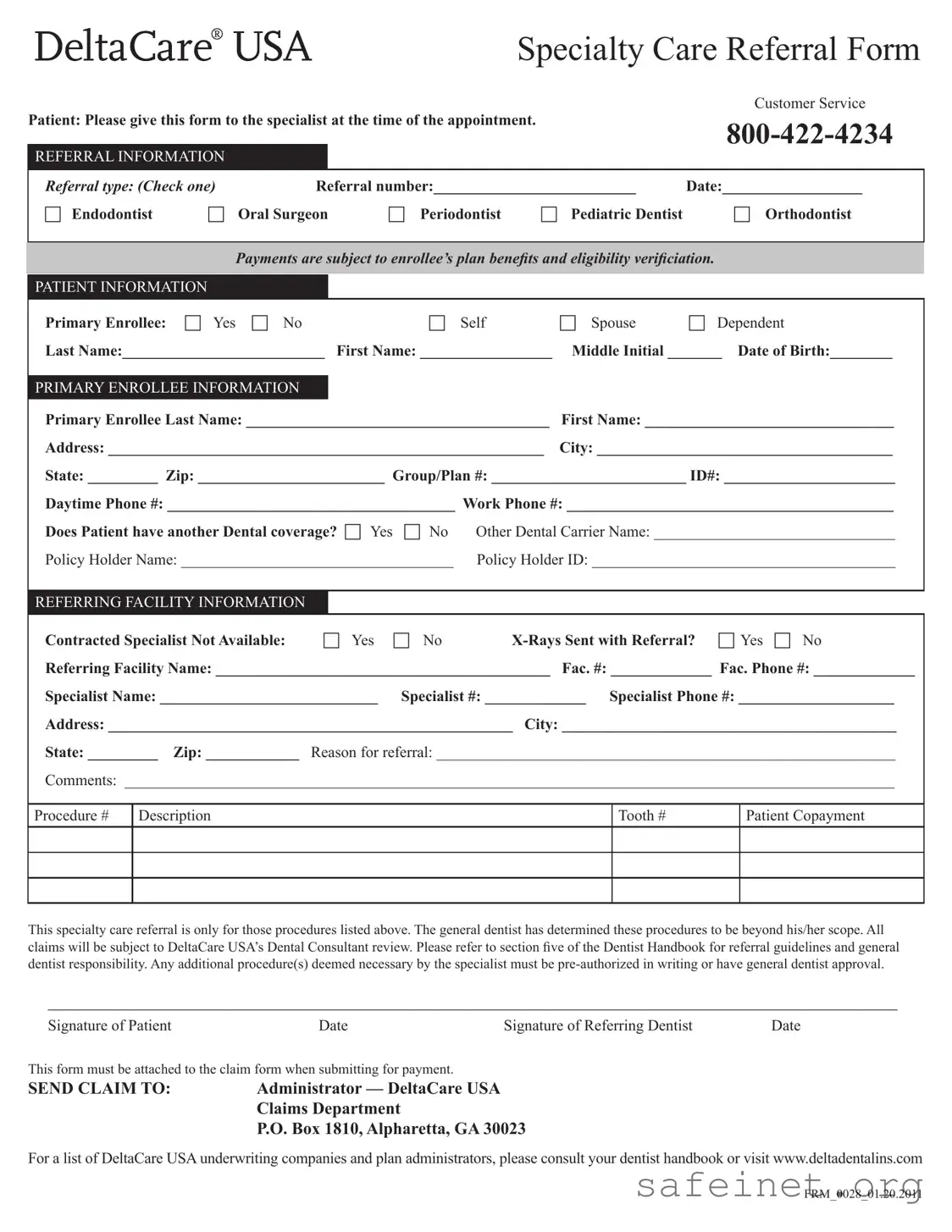
The Deltacare USA form is an essential document for patients seeking specialty dental care under their insurance plan. This form facilitates the referral process by capturing vital information needed for the appointment with a specialist. Patients must provide details such as their name, date of birth, and contact information, along with the primary enrollee's information. The form requires the referring dentist to specify the type of specialty care needed, whether it be for an endodontist, oral surgeon, or orthodontist, among others. Additionally, it addresses important aspects like the patient's other dental coverage, if applicable, and whether x-rays are included with the referral. The document also emphasizes that any procedures beyond the initial referral must receive prior authorization from the general dentist. To ensure proper processing, the completed form must be attached to the claim when submitting for payment. Overall, the Deltacare USA form streamlines communication between patients, general dentists, and specialists, helping to ensure that individuals receive the necessary dental care efficiently and effectively.
| Fact Name | Description |
|---|---|
| Referral Purpose | This form is designed for patients to provide necessary information to specialists at the time of their appointment. |
| Patient Information | Patients must fill out personal details, including their name, date of birth, and primary enrollee information, to ensure proper processing. |
| Specialist Information | Patients need to indicate the type of specialist they are being referred to, such as an endodontist or orthodontist. |
| Governing Laws | This form is governed by state-specific laws regarding dental care and insurance claims, which vary by state. |
Completing the Deltacare USA form is an essential step in ensuring your referral to a specialist is processed smoothly. Follow the steps below carefully to provide all necessary information accurately.
What is the purpose of the DeltaCare USA Specialty Care Referral Form?
The DeltaCare USA Specialty Care Referral Form is designed to facilitate referrals from general dentists to specialists. When a general dentist identifies a need for specialized treatment, they complete this form to ensure that the patient receives the appropriate care. It helps streamline the process, ensuring that both the patient and the specialist have the necessary information at the time of the appointment.
Who should fill out the DeltaCare USA form?
This form should be filled out by the referring dentist. They will provide details about the patient, the type of specialty care needed, and any relevant information about the referring facility. Patients are encouraged to bring the completed form to their specialist appointment to ensure that the specialist has all the necessary details for their treatment.
What information do I need to provide on the form?
You will need to provide several key pieces of information, including the patient's name, date of birth, and contact details. Additionally, the referring dentist must include their information, the type of specialist being referred to, and the reason for the referral. If the patient has other dental coverage, that information should also be noted on the form.
What happens if I do not have the referral form at my specialist appointment?
It is important to bring the referral form to your appointment. If you do not have it, the specialist may not have the necessary information to proceed with your treatment. This could lead to delays or the need for rescheduling. Always check with your referring dentist to ensure you have the form ready before your appointment.
Can additional procedures be performed without prior authorization?
No, any additional procedures that the specialist deems necessary must be pre-authorized in writing or approved by the referring dentist. This ensures that all treatments are covered under your plan and helps avoid unexpected costs. Always discuss any potential additional treatments with your specialist and referring dentist before proceeding.
Where should I send the completed claim form?
Once the treatment is completed, the claim form, along with the DeltaCare USA Specialty Care Referral Form, should be sent to the DeltaCare USA Claims Department at P.O. Box 1810, Alpharetta, GA 30023. Make sure to keep a copy for your records and check that all information is accurate to avoid any processing delays.
Failing to check the appropriate referral type. Make sure to select one option that accurately reflects the specialist you are referring to.
Omitting patient information. Ensure that all fields, including last name, first name, and date of birth, are filled out completely.
Not providing the primary enrollee information. Include the primary enrollee's full name and contact details to avoid processing delays.
Forgetting to indicate if the patient has other dental coverage. This information is crucial for verifying eligibility and benefits.
Neglecting to fill out the referring facility information. Include the name, phone number, and address of the referring facility to ensure proper communication.
Leaving out the reason for referral. Clearly state why the referral is necessary to help the specialist understand the patient's needs.
Not signing and dating the form. Both the patient and the referring dentist must provide their signatures to validate the referral.
Failing to attach the form to the claim submission. Remember that this form must be included when submitting claims for payment to ensure processing.
When dealing with dental care and insurance, several forms and documents often accompany the Deltacare USA form. Each serves a specific purpose in the referral and claims process. Here’s a brief overview of some commonly used documents.
Understanding these forms can help streamline the process of obtaining dental care and ensure that all necessary documentation is in order. Keeping everything organized will make your experience smoother and less stressful.
The Deltacare USA form is similar to the Medical Referral Form, which is used in healthcare settings to refer patients to specialists. This form collects essential patient information, including the referring physician's details and the specialist's information. Like the Deltacare USA form, it requires the reason for the referral and may also include insurance information to verify coverage before the patient sees the specialist.
Another document that shares similarities is the Dental Referral Form. This form is specifically designed for dental practices and includes sections for patient demographics, referring dentist details, and the specialist's information. Both forms aim to facilitate the referral process, ensuring that all necessary information is communicated effectively to the specialist for proper care.
The Insurance Pre-Authorization Form is also comparable. This document is used to obtain approval from an insurance company before a patient receives certain treatments. Like the Deltacare USA form, it requires detailed patient and provider information, as well as the specific services being requested. This ensures that the insurance company can verify eligibility and coverage before the procedure takes place.
Similar to the Deltacare USA form, the Patient Registration Form is often used in medical and dental offices. This form collects basic information about the patient, including their insurance details and emergency contact information. Both forms serve to gather necessary data for patient management and ensure that the office has the correct information on file.
The Authorization for Release of Information Form also bears resemblance to the Deltacare USA form. This document allows healthcare providers to share a patient's medical information with other professionals. It typically requires the patient's signature and details about the information being shared, similar to how the Deltacare USA form requires patient and provider signatures for referrals.
The Consent for Treatment Form is another document that is similar in purpose. This form is used to obtain a patient's consent before treatment can begin. Like the Deltacare USA form, it requires patient identification and may include details about the treatment being performed, ensuring that the patient understands what to expect.
The Referral for Specialist Consultation Form is closely related as well. This form is used when a primary care provider refers a patient to a specialist for further evaluation. It includes patient demographics and the reason for the referral, akin to the Deltacare USA form, which also emphasizes the need for clear communication regarding the patient's care.
The Claim Submission Form is another document that parallels the Deltacare USA form. This form is used to submit claims to insurance companies for reimbursement of medical or dental services rendered. It requires detailed patient information, provider details, and the services provided, similar to the referral process outlined in the Deltacare USA form.
Lastly, the Treatment Plan Form is similar in that it outlines the proposed treatment for a patient. This form includes patient information, details about the recommended procedures, and associated costs. Both the Treatment Plan Form and the Deltacare USA form serve to inform patients about their care and ensure that all necessary approvals are in place before treatment begins.
When filling out the DeltaCare USA form, it is important to follow certain guidelines to ensure accuracy and efficiency. Here are nine things you should and shouldn't do:
When dealing with the DeltaCare USA form, misunderstandings can lead to confusion and delays. Here are ten common misconceptions clarified for your understanding:
Understanding these misconceptions can help you navigate the DeltaCare USA referral process more effectively. Always consult with your dentist or insurance provider if you have questions or need further clarification.
When it comes to filling out and using the DeltaCare USA Specialty Care Referral Form, several important points should be kept in mind. Understanding these key takeaways can help ensure a smoother process for both patients and specialists.
By keeping these key takeaways in mind, patients can facilitate a more efficient referral process, ultimately leading to better dental care outcomes.