The DD 2870 form serves as a crucial document for various individuals, particularly those connected to the military and veterans' affairs. This form is integral for requesting health care services as well as for disclosing the rights and responsibilities that accompany specific medical treatments and benefits. By completing the DD 2870, individuals can authorize the release of their healthcare information, ensuring that necessary records are shared among authorized medical personnel. Additionally, the form includes provisions that protect the rights of patients regarding their personal health information. It’s important for service members and veterans to understand the implications of this form, including how to properly fill it out and where to submit it, as these details can significantly impact their access to essential health care services. Furthermore, understanding the context in which this form is utilized can help demystify its importance and ensure that individuals make informed decisions about their health care needs.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
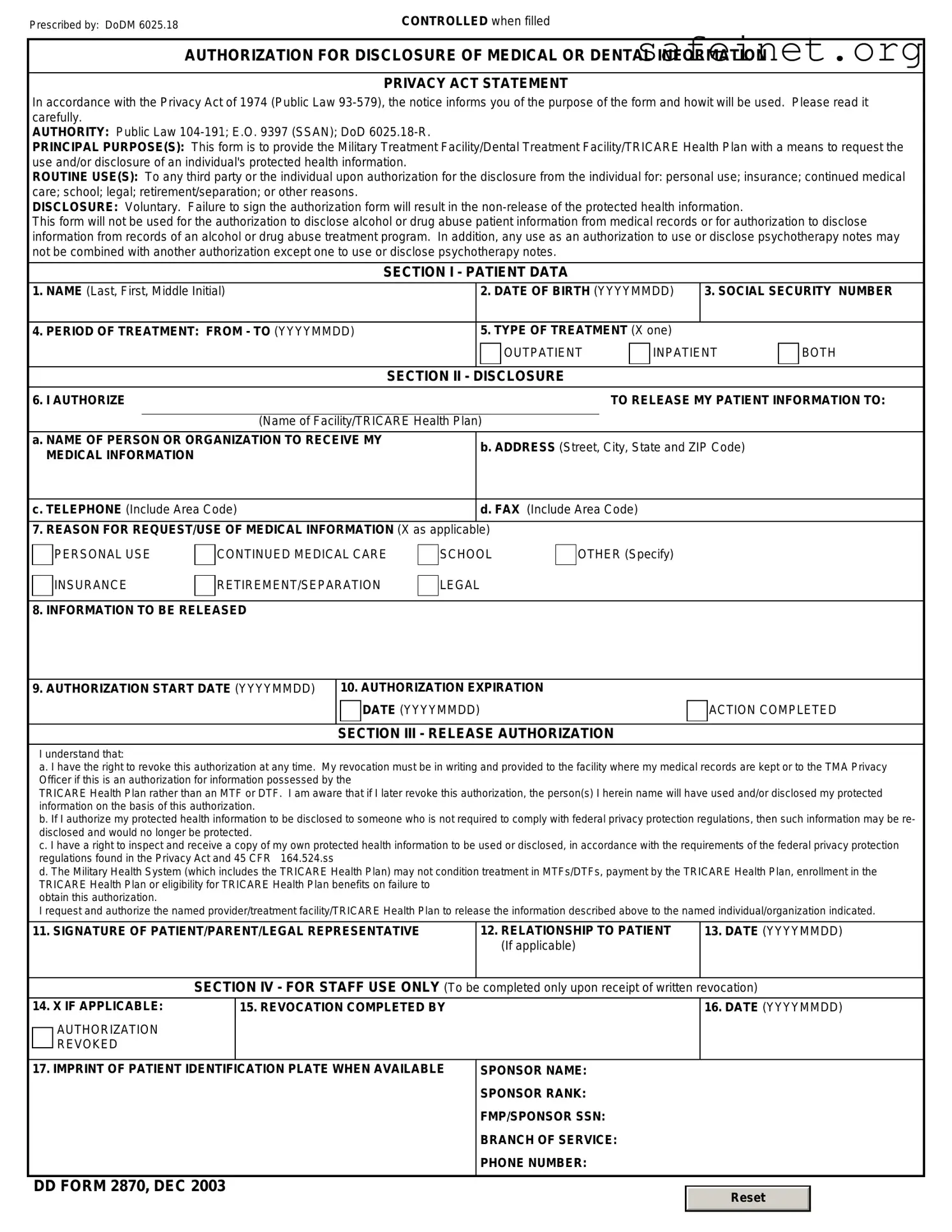
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Purpose | The DD 2870 form is used to request access to or copy of military personnel records. |
| Eligibility | Active duty service members, veterans, and eligible family members can use this form. |
| Submission Method | The completed form can be submitted online, by mail, or via fax, depending on the specific request. |
| Privacy Act Compliance | This form adheres to the Privacy Act of 1974, ensuring the protection of personal information. |
| Processing Time | Requests may take several weeks to process, depending on the complexity and volume of requests at that time. |
| State-Specific Laws | Some states have additional regulations regarding access to military records; for instance, California adheres to the Family Rights and Privacy Act. |
| Form Availability | The DD 2870 form is available through the official Department of Defense and National Archives websites. |
Filling out the DD 2870 form is a vital step in the process of submitting a request for a specific benefit or service. Completing this form accurately helps ensure that your application moves forward smoothly and that the right information is considered for your request. After filling it out, you will typically submit it to the relevant agency or office, which will then review your application and respond accordingly.
What is the DD 2870 form?
The DD 2870 form, also known as the “Authorization for Disclosure of Medical or Dental Information,” is used within the Department of Defense to obtain consent from patients for the release of their medical or dental records. This form ensures that service members, their dependents, and other eligible individuals can manage whom their health information is shared with, further protecting their privacy and ensuring adherence to regulations regarding sensitive health data.
Who needs to fill out the DD 2870 form?
This form is primarily required by service members, their family members, and certain eligible veterans who wish to authorize the release of their health information. If you need your records forwarded to a healthcare provider, a family member, or for personal reasons, filling out this form is essential.
Where can I obtain the DD 2870 form?
The DD 2870 form can typically be found online through the official Department of Defense websites or military health service websites. Local military medical facilities may also provide hard copies of the form, which can be filled out in person if preferred. It's important to ensure you have the most current version, as procedures and forms may change.
What information do I need to provide on the DD 2870 form?
You will need to provide personal identifying information, such as your name, Social Security number, and contact information. Additionally, the specific details about what medical or dental information you want disclosed will need to be included. It’s important to specify who you are authorizing to receive this information, along with their contact details.
How long does it take to process the DD 2870 form?
The processing time can vary based on the workload of the medical facility and the specifics of the requests being made. Generally, once submitted, it should take anywhere from a few days to a couple of weeks for the release of your information. For urgent requests, it might be beneficial to follow up with the appropriate medical records office.
Can I revoke my authorization after submitting the DD 2870 form?
Yes, you can revoke your authorization at any time. To do this, you'll need to provide a written notice to the office that currently has your signed DD 2870 form. Once your authorization is revoked, they will stop sharing any further information. However, any information that has already been shared prior to your revocation remains unaffected.
Is my health information safe after using the DD 2870 form?
While the DD 2870 form facilitates the sharing of your health information, it’s important to understand that the safety of this information depends largely on how well the receiving party protects your data. Ensure you authorize the release of your information to a trusted individual or healthcare provider, as they are responsible for maintaining its confidentiality after transfer.
Incomplete Information: Many individuals fail to provide all required personal information. Ensure that names, addresses, and contact details are fully filled out.
Incorrect Social Security Number: Entering an incorrect Social Security number can lead to significant delays. Double-check this detail to avoid issues.
Signature Errors: Missing a signature or providing an illegible one often results in rejection of the form. Sign clearly and in the designated areas.
Not Following Instructions: Each section of the DD 2870 has specific instructions. Ignoring these can lead to misunderstandings about what information is required.
Forgetting to Date the Form: Failing to date the completed form may create complications. Always include the date of submission.
Incorrect Form Version: Submitting an outdated version of the DD 2870 can cause delays or rejections. Verify that you are using the most current edition.
Neglecting to Include Supporting Documents: Some requests require additional documentation. Be sure to check if any supporting documents are needed and include them.
Not Keeping Copies: Failing to make copies of the completed form can be problematic. Always keep a copy for your records before sending it off.
Submitting to the Wrong Address: Ensure that the form is sent to the correct destination. Double-check the submission address to prevent any delays.
The DD 2870 form, which is utilized to authorize the release of medical, dental, or other personal information, is often accompanied by several important documents that support the process of obtaining this information. Understanding these additional forms can help streamline the procedure and ensure that all necessary permissions are granted. Below is a list of some forms commonly used alongside the DD 2870.
Using these forms in conjunction with the DD 2870 can significantly enhance the efficiency of accessing essential personal and medical information. Each document plays a vital role in ensuring that individuals maintain control over their own data, thus promoting transparency and trust in the military and healthcare systems.
The DD 214 is a form issued by the U.S. Department of Defense. It serves as an official record of a military service member's time in the military. Like the DD 2870, the DD 214 is crucial for veterans seeking benefits, as it provides necessary details such as discharge status and service dates. Both forms involve personal information and must be accurately completed to facilitate access to the appropriate resources and support for veterans.
The SF-180, or Request Pertaining to Military Records, is another important document. This form allows individuals to request copies of their military records from the National Archives. Similar to the DD 2870, the SF-180 requires specific personal details and the purpose of the request. Both forms play significant roles in ensuring veterans can obtain their service records to claim benefits or for personal reasons.
The VA Form 21-526EZ, Application for Disability Compensation and Related Compensation Benefits, is also comparable. This form enables veterans to apply for disability benefits due to injuries or illnesses sustained during service. Much like the DD 2870, it involves detailed personal information and is essential for accessing veterans' benefits. Completing both forms correctly is vital for a smooth application process.
The VA Form 10-5345, Request for and Authorization to Release Medical Records or Health Information, is another document that shares similarities. This form is used to authorize the release of a veteran's medical records to the Department of Veterans Affairs. Similar to the DD 2870, the VA Form 10-5345 requires clear information about the individual and the purpose of the request. Both forms are designed to protect personal information while ensuring veterans receive the necessary support and services.
When filling out the DD 2870 form, it's essential to pay attention to certain practices that can ensure a smoother process. Here’s a list of things to do and avoid:
By adhering to these guidelines, you can help ensure that your submission is efficient and meets all necessary requirements.
The DD 2870 form is only for military personnel. This form is not limited to just military members. It can be used by eligible family members and dependents as well, allowing them to access healthcare services provided by the military health system.
Submitting the DD 2870 form guarantees access to medical services. While submitting the form is a necessary step to request healthcare, it does not guarantee that services will be provided. Eligibility and availability depend on various factors, including specific healthcare needs and the current capacity of facilities.
The DD 2870 form cannot be updated once submitted. Individuals have the ability to update their information on the form even after submission. Changes in personal circumstances, such as address or contact information, should be communicated to ensure that records remain accurate.
Only certain types of medical services require the DD 2870 form. This form is applicable for a wide range of medical services, not just specific types. It covers various healthcare needs, facilitating access to comprehensive healthcare options under the military health system.
The DD 2870 form is an important document for individuals seeking certain benefits or services. Here are some key takeaways to consider when filling it out:
Filling out the DD 2870 form with care can facilitate the smooth processing of your request. Make sure to keep these takeaways in mind as you navigate through the form.
Cash Receipt Format - Instrumental in managing daily cash intake efficiently.
House Load Calculation - Essential for ensuring safety and compliance with electrical codes.
Choice Reservations - Providing all requested information ensures compliance with the hotel’s policies.