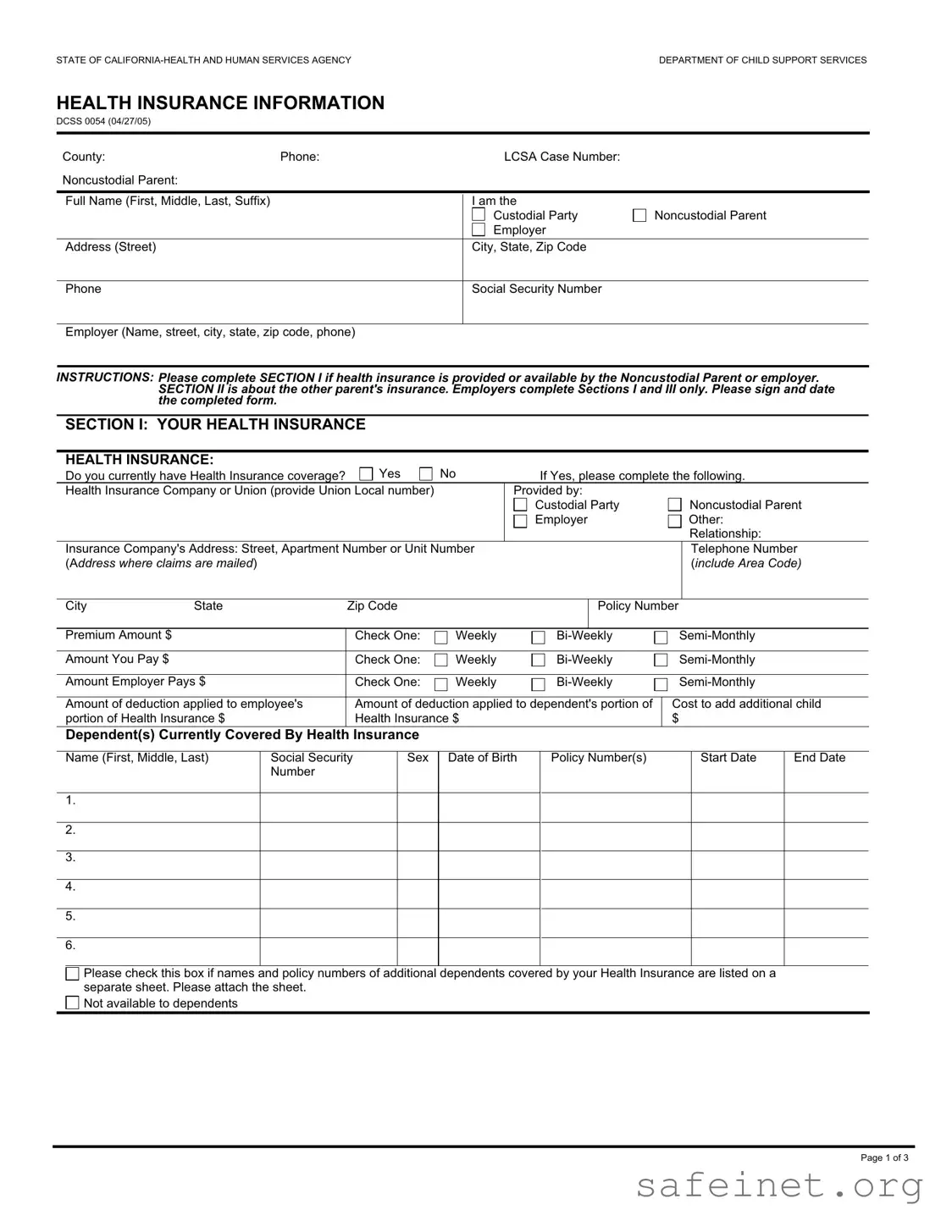
The DCSS 0054 form, officially titled "Health Insurance Information," plays a crucial role in the management of child support cases in California. Designed by the Department of Child Support Services, this form facilitates the collection of essential health insurance details from both custodial and noncustodial parents. It consists of multiple sections that capture information about the health, dental, and vision insurance coverage available to children involved in custody arrangements. Parents are required to provide their personal details, including Social Security numbers, and specify their insurance coverage status. The form also prompts for information about the other parent's insurance, ensuring that all relevant health insurance options are explored. By completing this form, parents help ensure that their children have access to necessary medical care, which is a fundamental aspect of child support obligations. Furthermore, the DCSS 0054 emphasizes the importance of timely communication with the local child support agency regarding any changes in insurance status, thereby promoting transparency and accountability in child support arrangements.
| Fact Name | Description |
|---|---|
| Form Purpose | The DCSS 0054 form is used to collect health insurance information for children involved in child support cases in California. |
| Governing Law | This form is governed by the California Family Code, specifically sections related to child support and health insurance obligations. |
| Sections Overview | The form consists of three sections: health insurance details of the noncustodial parent, information about the other parent's insurance, and a confirmation of insurance coverage. |
| Required Information | It requires personal details, insurance company information, and specifics about the coverage for the child(ren). |
| Privacy Statement | The form includes a privacy statement that informs individuals about the collection and use of their personal information, ensuring compliance with federal and state privacy laws. |
Completing the DCSS 0054 form is essential for providing health insurance information related to child support. Follow the steps below to ensure that all necessary information is accurately filled out. Make sure to review your responses before submitting the form.
What is the DCSS 0054 form?
The DCSS 0054 form is used in California by the Department of Child Support Services to collect information regarding health insurance coverage for children involved in child support cases. This form helps ensure that children have access to necessary medical care and that the responsible parties are identified for insurance purposes.
Who needs to complete the DCSS 0054 form?
The form must be completed by the noncustodial parent or their employer if they provide health insurance coverage. Additionally, custodial parties may also need to provide information about their own health insurance coverage and that of the children.
What information is required in Section I of the form?
Section I requires details about the health insurance provided by the noncustodial parent or their employer. This includes the name of the insurance company, policy numbers, premium amounts, and information about covered dependents. The section also asks about dental and vision insurance coverage if applicable.
What should I do if I do not have health insurance?
If health insurance is not available, the form allows you to indicate this. You will need to explain why coverage is unavailable, such as being part-time, seasonal, or having refused enrollment. It is important to notify the local child support agency if insurance becomes available in the future.
What is the purpose of Section II of the form?
Section II is focused on the health insurance coverage provided by the other parent. It asks whether the other parent provides health, dental, or vision insurance for the children. If they do, specific details about the insurance must be provided.
What happens if I do not have the insurance card at the time of filling out the form?
You can indicate on the form that you do not have the insurance card or information available at the moment. You will be required to send this information to the local child support agency as soon as you receive it from the insurance company.
Is there a privacy statement associated with the DCSS 0054 form?
Yes, the form includes a privacy statement that explains how the information collected will be used. It clarifies that personal information, including Social Security Numbers, is necessary for identification and communication purposes. The privacy statement outlines how this information may be shared in compliance with legal requirements.
What types of insurance coverage does the form inquire about?
The form inquires about health, dental, and vision insurance coverage. For each type of insurance, it asks for the insurance company's name, address, policy numbers, and details about premiums and coverage for dependents.
How should I submit the completed DCSS 0054 form?
The completed form should be signed and dated before submission. It can typically be sent to the local child support agency by mail or in person, depending on the agency's specific instructions.
Where can I find assistance if I have questions about completing the form?
If you have questions while completing the DCSS 0054 form, you can contact your local child support agency for assistance. They can provide guidance on how to fill out the form correctly and answer any specific questions you may have.
Incomplete Information: Many individuals fail to fill out all required sections of the DCSS 0054 form. Sections I, II, and III must be completed as applicable. Missing information can delay processing.
Incorrect Contact Information: Providing inaccurate phone numbers or addresses for the custodial or noncustodial parent can hinder communication. Always double-check these details before submitting.
Omitting Social Security Numbers: The form requires the Social Security Number of both parents and any dependents. Omitting this information can lead to complications in processing child support cases.
Failure to Sign and Date: A common oversight is neglecting to sign and date the form. Without a signature, the form is considered incomplete and may not be processed.
Not Attaching Additional Information: If there are more dependents than can be listed on the form, individuals often forget to attach a separate sheet. This can lead to incomplete records regarding insurance coverage.
The DCSS 0054 form, which collects health insurance information for child support purposes, is often accompanied by several other important documents. Each of these documents serves a specific purpose in the child support process, ensuring that all relevant information is accurately recorded and communicated. Below is a list of commonly used forms and documents that may be required alongside the DCSS 0054 form.
Each of these documents plays a crucial role in the child support process. By providing comprehensive information, they help ensure that the rights and responsibilities of both parents are clearly understood and upheld. Accurate documentation is key to effective communication between parents and the child support agency, ultimately benefiting the children involved.
The DCSS 0054 form is similar to the Child Support Worksheet, which is often used in child support cases. Both documents require detailed information about the financial circumstances of the parties involved. The Child Support Worksheet collects data on income, expenses, and other financial obligations to calculate the appropriate support amount. Like the DCSS 0054, it aims to ensure that children receive adequate financial support, but it focuses more on the overall financial picture rather than specifically on health insurance details.
Another document comparable to the DCSS 0054 is the Health Insurance Information form used in divorce proceedings. This form serves a similar purpose by gathering information about existing health insurance coverage for children. It requires parties to disclose their health insurance details, including policy numbers and coverage specifics. Both forms emphasize the importance of health insurance in child support cases, ensuring that children have access to necessary medical care.
The Medical Support Order is another document that shares similarities with the DCSS 0054 form. This order is issued by the court and mandates that one parent provide health insurance coverage for the child. Like the DCSS 0054, it aims to secure health insurance for the child, outlining the responsibilities of each parent. Both documents highlight the necessity of health insurance as part of a comprehensive child support plan.
The Declaration of Disclosure is also akin to the DCSS 0054 form in that it requires parties to disclose financial information, including insurance coverage. While the Declaration of Disclosure is broader in scope, it still emphasizes the need for transparency regarding health insurance. Both documents aim to ensure that all relevant information is available to the court for making informed decisions about child support and welfare.
The Child Support Agreement can be compared to the DCSS 0054 form as well. This agreement outlines the terms of child support, including health insurance provisions. Both documents serve to formalize the responsibilities of each parent regarding the child's welfare. They ensure that health insurance is addressed as part of the overall child support arrangement, thereby prioritizing the child's needs.
The Affidavit of Support is another document that bears resemblance to the DCSS 0054 form. This affidavit is often used in immigration cases to demonstrate financial support for a dependent. While its primary focus is different, it similarly requires detailed information about financial resources, including health insurance coverage. Both documents aim to provide a safety net for dependents, ensuring their health and well-being are taken into account.
The Parent's Health Insurance Information form is closely related to the DCSS 0054 form as it specifically collects data about health insurance coverage for children. This form requires parents to report their insurance details, similar to the DCSS 0054. Both documents are essential in establishing the availability of health care resources for children and ensuring that both parents fulfill their obligations regarding health insurance.
Lastly, the Child Custody Agreement often includes provisions for health insurance, making it similar to the DCSS 0054 form. This agreement outlines the custody arrangements and responsibilities of each parent, including who will provide health insurance for the child. Both documents emphasize the importance of health care access and detail the obligations of each parent to ensure that the child's health needs are met.
When filling out the DCSS 0054 form, it’s important to be careful and thorough. Here’s a list of things you should and shouldn’t do:
Here are seven common misconceptions about the DCSS 0054 form, along with clarifications for each:
Understanding these misconceptions can help ensure that the DCSS 0054 form is filled out accurately and submitted on time. This promotes the well-being of the children involved and helps maintain compliance with child support regulations.