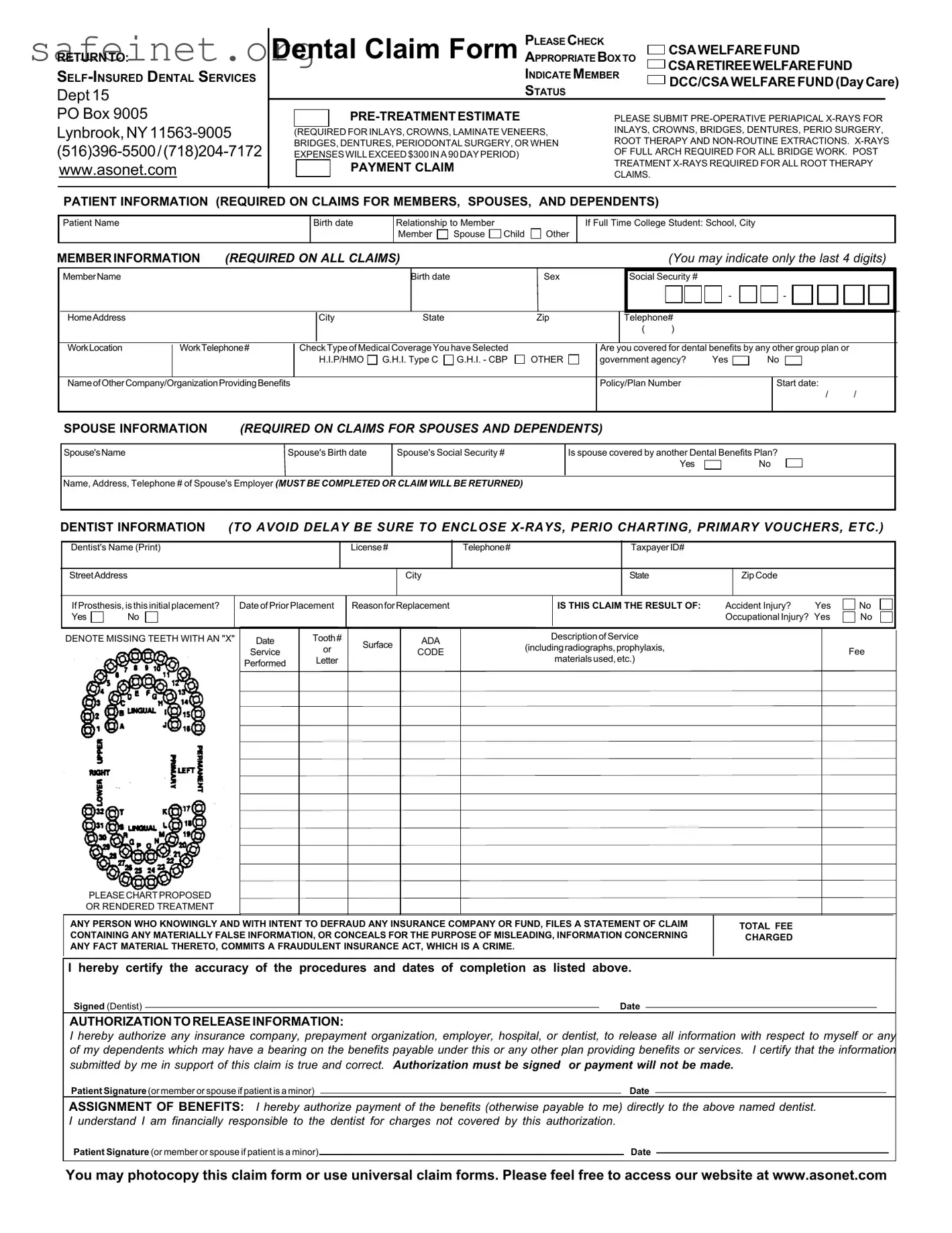
The Csa Dental form serves as a crucial document for individuals seeking dental benefits through various plans, including the CSA Welfare Fund and the CSA Retiree Welfare Fund. It allows members to submit claims for dental services, ensuring they receive appropriate reimbursement. Essential sections in the form include patient and member information, detailing the individual's relationship to the member, and any additional dental coverage through other insurance plans. The form also requires dentists to provide their information, including license details and the nature of treatments delivered. A pre-treatment estimate is necessary for certain procedures, accompanied by required X-rays that assist in accurately assessing treatment costs. Furthermore, the form addresses circumstances related to accidents or job injuries to clarify coverage entitlements. It is important for every section to be filled out thoroughly to prevent delays in payment. This structured document also includes signatures for authorization, ensuring the information provided is accurate and can be shared with relevant parties for processing claims. Understanding each aspect of this form is vital for timely and effective access to dental care benefits.
RETURNTO:
PLEASE CHECK
Dental Claim Form APPROPRIATE BOX TO  CSAWELFAREFUND
CSAWELFAREFUND
CSARETIREEWELFAREFUND
Dept 15
INDICATE MEMBER
STATUS
DCC/CSAWELFAREFUND(DayCare)
PO Box 9005
|
|
PLEASE SUBMIT |
||
|
|
|
INLAYS, CROWNS, BRIDGES, DENTURES, PERIO SURGERY, |
|
(REQUIRED FOR INLAYS, CROWNS, LAMINATE VENEERS, |
||||
ROOT THERAPY AND |
||||
BRIDGES, DENTURES, PERIODONTAL SURGERY, OR WHEN |
||||
OF FULL ARCH REQUIRED FOR ALL BRIDGE WORK. POST |
||||
EXPENSES WILLEXCEED$300INA 90 DAY PERIOD) |
||||
TREATMENT |
||||
|
|
PAYMENT CLAIM |
||
|
|
CLAIMS. |
||
|
|
|
||
|
|
|
||
PATIENT INFORMATION (REQUIRED ON CLAIMS FOR MEMBERS, SPOUSES, AND DEPENDENTS)
Patient Name
Birth date
Relationship to Member |
|
|
Member |
Spouse |
Child |
Other
If Full Time College Student: School, City
MEMBERINFORMATION (REQUIRED ON ALL CLAIMS) |
(You may indicate only the last 4 digits) |
MemberName
Birth date |
Sex |
|
|
Social Security #
-
-
|
HomeAddress |
|
|
City |
State |
|
Zip |
|
Telephone# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
WorkLocation |
WorkTelephone# |
CheckTypeofMedicalCoverageYouhaveSelected |
|
Are you covered for dental benefits by any other group plan or |
|
|
|
|||||||||||
|
|
|
|
H.I.P/HMO |
G.H.I. Type C |
G.H.I. - CBP |
OTHER |
government agency? |
Yes |
|
No |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NameofOtherCompany/OrganizationProvidingBenefits |
|
|
|
|
|
Policy/Plan Number |
|
|
|
Start date: |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPOUSE INFORMATION (REQUIRED ON CLAIMS FOR SPOUSES AND DEPENDENTS)
Spouse'sName |
Spouse's Birth date |
Spouse's Social Security # |
|
|
|
Is spouse covered by another Dental Benefits Plan?
Yes |
|
No |
Name, Address, Telephone # of Spouse's Employer (MUST BE COMPLETED OR CLAIM WILL BE RETURNED)
DENTIST INFORMATION (TO AVOID DELAY BE SURE TO ENCLOSE
Dentist's Name (Print)
License#
Telephone#
TaxpayerID#
StreetAddress
City
State
ZipCode
IfProsthesis,isthisinitialplacement? |
|
DateofPrior Placement |
ReasonforReplacement |
|
IS THIS CLAIM THE RESULT OF: |
Accident Injury? |
Yes |
No |
|||
Yes |
No |
|
|
|
|
|
|
|
Occupational Injury? |
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
DENOTE MISSING TEETH WITH AN "X" |
Date |
Tooth# |
Surface |
ADA |
DescriptionofService |
|
|
|
|||
|
|
|
Service |
or |
CODE |
(includingradiographs,prophylaxis, |
|
|
Fee |
||
|
|
|
|
|
|
||||||
|
|
|
Performed |
Letter |
|
|
|
materialsused,etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASECHARTPROPOSED
OR RENDERED TREATMENT
ANY PERSON WHO KNOWINGLY AND WITH INTENT TO DEFRAUD ANY INSURANCE COMPANY OR FUND, FILES A STATEMENT OF CLAIM CONTAINING ANY MATERIALLY FALSE INFORMATION, OR CONCEALS FOR THE PURPOSE OF MISLEADING, INFORMATION CONCERNING ANY FACT MATERIAL THERETO, COMMITS A FRAUDULENT INSURANCE ACT, WHICH IS A CRIME.
TOTAL FEE CHARGED
I hereby certify the accuracy of the procedures and dates of completion as listed above.
Signed (Dentist) |
|
Date |
|
AUTHORIZATIONTORELEASEINFORMATION:
I hereby authorize any insurance company, prepayment organization, employer, hospital, or dentist, to release all information with respect to myself or any of my dependents which may have a bearing on the benefits payable under this or any other plan providing benefits or services. I certify that the information submitted by me in support of this claim is true and correct. Authorization must be signed or payment will not be made.
Patient Signature(or member or spouse if patient is a minor) |
|
Date |
|
ASSIGNMENT OF BENEFITS: I hereby authorize payment of the benefits (otherwise payable to me) directly to the above named dentist. I understand I am financially responsible to the dentist for charges not covered by this authorization.
Patient Signature (or member or spouse if patient is a minor) |
|
Date |
You may photocopy this claim form or use universal claim forms. Please feel free to access our website at www.asonet.com
| Fact Name | Description |
|---|---|
| Purpose of the Form | The CSA Dental Form is used to submit claims for dental services for members and their dependents. |
| Member Eligibility | Eligible members include members, their spouses, and dependents who have dental coverage. |
| Pre-Treatment Requirements | X-rays are required for specific treatments, including crowns and dentures, prior to approval. |
| Missing Teeth Notation | Members must denote missing teeth by marking them with an "X" on the form. |
| Fraud Warning | Signing the form certifies that no false information has been provided, as fraudulent claims are criminal offenses. |
| Authorization for Release of Information | Members must authorize the release of their information to process claims and ensure payment. |
| Direct Payment Option | Members can direct benefit payments to their dentist by signing the assignment of benefits section. |
| Contact Information | The form provides contact details for inquiries, including phone numbers and a website. |
| Government Regulations | This form may be subject to state-specific governing laws related to dental claims, varying by state. |
| Submission Instructions | Claims must be submitted to the designated mailing address, including all necessary supporting documents. |
Filling out the CSA Dental form accurately is crucial for ensuring that your dental claims are processed efficiently. To assist you, the following steps will guide you through the process. Be sure to have all necessary information at hand, and take your time to fill out each section carefully before submitting the form.
Once you have completed the form, double-check for completeness and accuracy. Any missing information could result in processing delays. After reviewing, submit your form to the address provided on the top for timely processing.
What is the purpose of the CSA Dental form?
The CSA Dental form is primarily designed to submit dental claims for reimbursement. It allows members, their spouses, and dependents to receive payment for dental services provided by a participating dentist. Proper completion of the form is necessary to ensure timely processing of claims.
What information is required on the CSA Dental form?
To complete the CSA Dental form, you must provide specific details about the patient, member, and dentist. This includes names, dates of birth, relationships, and contact information. Additionally, any existing medical coverage must be specified. The dentist's information and details of the dental treatment performed are also required to process the claim.
Are there any specific documentation requirements for submitting a claim?
Yes, certain documentation is necessary to prevent delays. You must attach preoperative X-rays for specific dental procedures like inlays, crowns, or bridges. Furthermore, periodontal surgery and root therapy claims require additional X-ray submissions. Ensure that all relevant documents are enclosed with the claim to facilitate proper evaluation.
How can I check the status of my submitted claim?
You can check the status of your claim by contacting the provided phone numbers on the form, either (516) 396-5500 or (718) 204-7172. You may also visit the official website at www.asonet.com for additional resources or information regarding your claims.
What should I do if my claim is denied or returned?
If your claim is denied or returned, review the reason for the decision provided by the insurance company. Ensure that all required fields were completed accurately and that all necessary documentation was included. If you find an error or need further clarification, don't hesitate to reach out to their customer service for assistance in resolving the issue.
What happens if the information on the form is incorrect?
Submitting incorrect information on the CSA Dental form may lead to delayed processing or denial of your claim. It is essential to double-check all entries for accuracy before submission. If you notice an error after submission, contact the insurance provider immediately to correct the information and provide any necessary documentation to prevent complications.
Incomplete Patient Information: Failing to provide all necessary details about the patient can delay claims. Information such as full name, date of birth, and relationship to the member must be complete. Double-check for accuracy, as omissions or errors may cause the claim to be rejected.
Missing Supporting Documentation: Submitting the form without required documents can be a significant mistake. For treatments like crowns or dentures, x-rays and other supporting materials are mandatory. Without these, claims may be delayed or denied.
Incorrect Member Information: Ensure that member details match those on file. Discrepancies in names, Social Security numbers, or other identifiers can complicate the claims process. It’s crucial to verify that all member-related information is consistent and accurately filled out.
Ignoring the Authorization Section: Not signing the authorization to release information can lead to claim denials. This section is essential to ensure that all relevant medical information is shared for the claim to be processed. Always make sure to read and understand what you are signing.
The CSA Dental Form is an essential document used to process dental claims. However, it is not used in isolation. Other forms and documents often accompany it to ensure that each aspect of the claim is handled properly. Here’s a list of additional forms that may be utilized along with the CSA Dental Form:
These forms work in conjunction with the CSA Dental Form to facilitate a thorough and efficient claims process. Understanding each document’s role can help ensure a smoother experience for patients seeking dental care. Properly completing and submitting these documents is crucial for timely reimbursement from insurance providers.
The Dental Patient Information Form is similar to the CSA Dental form in its purpose of collecting essential patient details. Both forms require the patient's name, birth date, and relationship to the member, ensuring that all necessary information is gathered for verification. The forms also emphasize the importance of accurate data by including provisions for additional questions regarding insurance coverage, making it easier to process claims efficiently.
The Dental Insurance Claim Form serves a function akin to the CSA Dental form, focusing on the submission of claims for dental benefits. Both documents require specific information about the patient, member, and provider to facilitate the claims process. They necessitate the inclusion of treatment codes and the corresponding fees, helping streamline the interaction between dental offices and insurance companies.
The Pre-Treatment Estimate Request mirrors the CSA Dental form by gathering details related to proposed dental services before treatment is performed. Each form stresses the need for x-rays and treatment plans to be submitted for approval, ensuring that the predicted costs align with the administrative criteria set by the insurance provider. By requiring pre-authorization, these forms aim to minimize misunderstandings about covered services.
The Universal Claim Form has similarities with the CSA Dental form in that it can be utilized across multiple insurance providers. Like the CSA form, it collects important patient and treatment information, allowing for consistent processing of claims. The universal nature of this form means it encourages efficiency and standardization in filing claims across various health plans.
The Medical History Form is comparable to the CSA Dental form as both documents gather crucial background information regarding the patient. This information helps ensure that the dental provider understands any pre-existing conditions or past treatments that might affect the current claims process. Furthermore, both forms may refer to the patient’s eligibility for benefits under different circumstances.
The Treatment Authorization Form reflects the CSA Dental form in its purpose of documenting the need for prescribed dental services. Both require patient signatures for consent, emphasizing the importance of agreement on treatment plans and potential costs before services are rendered. This process aids in protecting both the patient and provider from future disputes related to treatment coverage.
The Patient Consent Form is similar to the CSA Dental form in that it secures approval from the patient or guardian for treatment and any necessary disclosures to insurance providers. Both documents underscore the importance of informed consent, protecting the rights of patients while ensuring that dental teams comply with legal and ethical obligations.
The Employee Benefits Enrollment Form parallels the CSA Dental form by often including dental coverage options as part of overall employee benefits. Information regarding dependents and their eligibility for benefits forms a crucial aspect of both documents. This alignment assures that all eligible family members are accounted for when filing claims or utilizing services.
The Continuity of Care Form shares similarities with the CSA Dental form in that it keeps track of ongoing treatments and required follow-ups. Both forms may request information on previous dental work and the continuing requirements for care. This type of documentation ensures that comprehensive information is available, minimizing lapses in treatment and enhancing patient outcomes.
Lastly, the Secondary Insurance Claim Form reflects aspects of the CSA Dental form in its focus on multiple insurance claims. Similar to the CSA form, it requires detailed information related to the primary and secondary coverage, ensuring that benefits are coordinated effectively across different plans. This collaboration is vital for ensuring patients receive the appropriate level of coverage for their dental services.
When filling out the CSA Dental form, it is crucial to be thorough and accurate. Here are some essential do's and don'ts to ensure the process goes smoothly.
Many people have misunderstandings about the CSA Dental form. Here are five common misconceptions and explanations to clarify them.
This is not true. The CSA Dental form can be used by both members and their dependents, including spouses and children. It is designed for anyone who qualifies for the dental benefits offered by the program.
Contrary to this belief, pre-treatment estimates are often required for many procedures, even those that seem minor. For example, X-rays must be included for treatments like crowns and extractions, regardless of their perceived simplicity.
This misconception can lead to delays or rejection of claims. X-rays are mandatory for specific procedures and should be submitted alongside the form to avoid complications.
This is incorrect. While certain sections must be completed by the dentist, the patient or member can fill out their information, such as personal details and insurance coverage, making the process collaborative.
Actually, signatures are crucial for authorization. The form cannot be processed without the patient's signature, which certifies that all the information is accurate and permits the release of necessary information to the insurance company.
When filling out the CSA Dental form, it is essential to ensure accuracy and completeness. Here are key takeaways to consider:
Following these guidelines will simplify your experience when using the CSA Dental form. Proper completion ensures that your dental claims are handled efficiently and effectively.