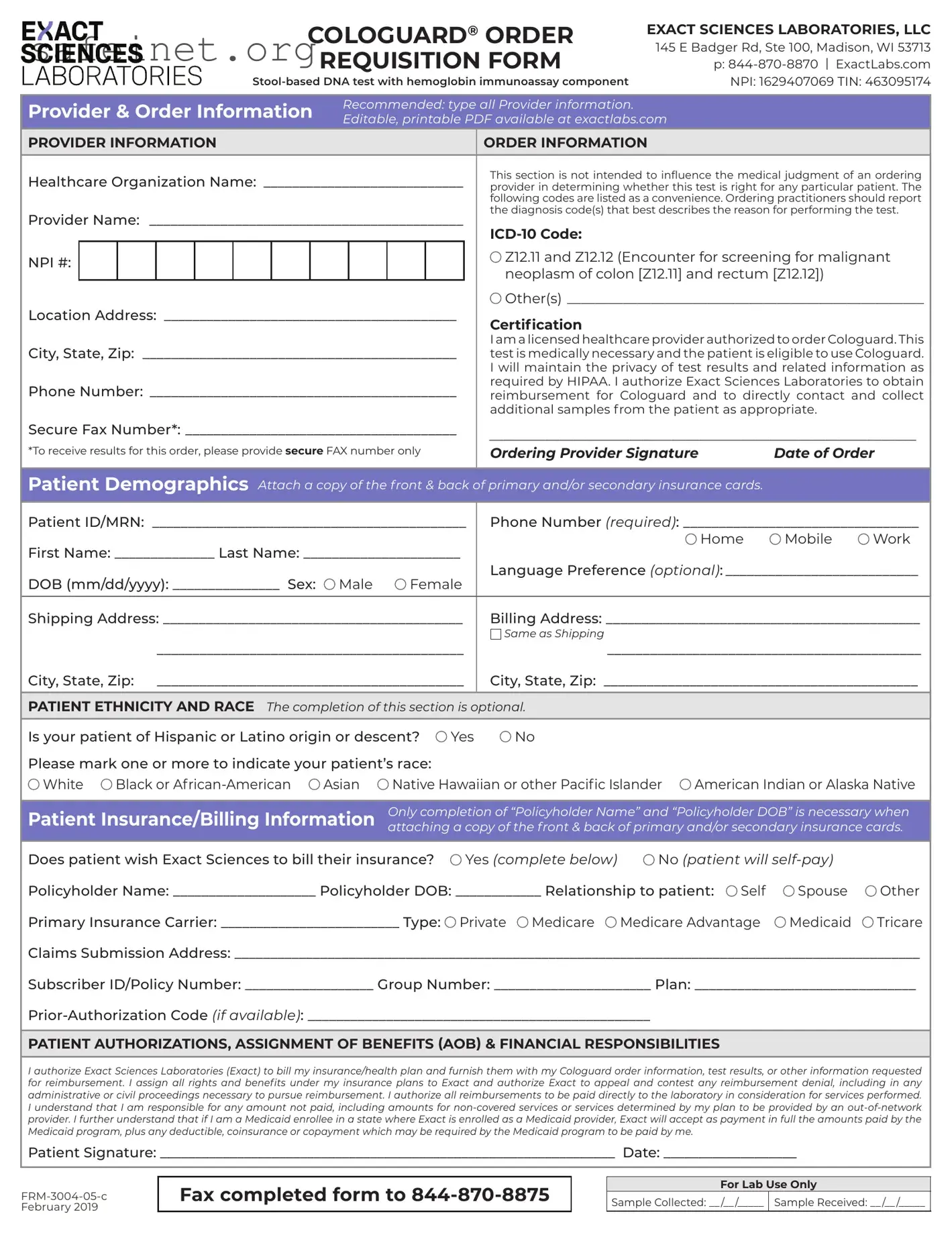
The Cologuard Order Form serves as an essential tool for healthcare providers looking to order the innovative stool-based DNA test designed to detect colorectal cancer. This streamlined form, available in a printable PDF format, collects vital information about both the provider and the patient. It starts by capturing detailed provider information, including the healthcare organization’s name, NPI number, and contact details, which are all critical for accurate processing. Next, the order information prompts the provider to select appropriate diagnosis codes that justify the test's medical necessity, helping to ensure coverage and compliance with insurance requirements. Importantly, the form includes a section for patient demographics, allowing for the collection of data such as date of birth, sex, and language preference. Additionally, there’s space to document insurance and billing information, which can simplify reimbursement processes. This comprehensive structure isn't just administrative; it acknowledges the healthcare provider's responsibility to maintain patient confidentiality as mandated by HIPAA. Understanding each component of the Cologuard Order Form can enhance communication between patients and providers, ultimately facilitating more effective screening for colorectal cancer.
|
|
|
|
|
|
|
COLOGUARD® ORDER |
EXACT SCIENCES LABORATORIES, LLC |
|||||||||
|
|
|
|
|
|
|
|
|
REQUISITION FORM |
145 E Badger Rd, Ste 100, Madison, WI 53713 |
|||||||
|
|
|
|
|
|
|
|
|
|
p: |
|||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
NPI: 1629407069 TIN: 463095174 |
||||||||||
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Provider & Order Information |
Recommended: type all Provider information. |
|
|
||||||||||||||
Editable, printable PDF available at exactlabs.com |
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
PROVIDER INFORMATION |
|
|
|
|
|
ORDER INFORMATION |
|
||||||||||
Healthcare Organization Name: _____________________________ |
This section is not intended to influence the medical judgment of an ordering |
||||||||||||||||
provider in determining whether this test is right for any particular patient. The |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
following codes are listed as a convenience. Ordering practitioners should report |
|||
Provider Name: _____________________________________________ |
the diagnosis code(s) that best describes the reason for performing the test. |
||||||||||||||||
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NPI #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Z12.11 and Z12.12 (Encounter for screening for malignant |
|||
|
|
|
|
|
|
|
|
|
|
|
|
neoplasm of colon [Z12.11] and rectum [Z12.12]) |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Location Address: __________________________________________ |
Other(s)____________________________________________________ |
||||||||||||||||
Certification |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City, State, Zip: _____________________________________________ |
I am a licensed healthcare provider authorized to order Cologuard. This |
||||||||||||||||
test is medically necessary and the patient is eligible to use Cologuard. |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I will maintain the privacy of test results and related information as |
|||
Phone Number: ____________________________________________ |
required by HIPAA. I authorize Exact Sciences Laboratories to obtain |
||||||||||||||||
reimbursement for Cologuard and to directly contact and collect |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
additional samples from the patient as appropriate. |
|||
Secure Fax Number*: ______________________________________ |
_____________________________________________________________ |
||||||||||||||||
*To receive results for this order, please provide secure FAX number only |
|||||||||||||||||
Ordering Provider Signature |
Date of Order |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Demographics Attach a copy of the front & back of primary and/or secondary insurance cards.
Patient ID/MRN: ____________________________________________ |
Phone Number (required): _________________________________ |
||||||||||
First Name: ______________ Last Name: ______________________ |
|
|
Home |
Mobile |
Work |
||||||
Language Preference (optional):____________________________ |
|||||||||||
DOB (mm/dd/yyyy): _______________ Sex: |
Male |
Female |
|||||||||
|
|
|
|
|
|
||||||
Shipping Address: __________________________________________ |
Billing Address: ____________________________________________ |
||||||||||
|
|
|
|
|
Same as Shipping |
|
|
|
|
|
|
|
___________________________________________ |
____________________________________________ |
|||||||||
City, State, Zip: ___________________________________________ |
City, State, Zip: ____________________________________________ |
||||||||||
|
|
|
|
|
|
|
|||||
PATIENT ETHNICITY AND RACE The completion of this section is optional. |
|
|
|
|
|
||||||
Is your patient of Hispanic or Latino origin or descent? |
Yes |
No |
|
|
|
|
|
||||
Please mark one or more to indicate your patient’s race: |
|
|
|
|
|
|
|
||||
White |
Black or |
Asian |
Native Hawaiian or other Pacific Islander |
American Indian or Alaska Native |
|||||||
|
|
|
|
|
|||||||
Patient Insurance/Billing Information |
Only completion of “Policyholder Name” and “Policyholder DOB” is necessary when |
||||||||||
attaching a copy of the front & back of primary and/or secondary insurance cards. |
|||||||||||
|
|
|
|
|
|||||||
Does patient wish Exact Sciences to bill their insurance? |
Yes (complete below) |
No (patient will |
|
||||||||
Policyholder Name: ____________________ Policyholder DOB: ____________ Relationship to patient: |
Self |
Spouse |
Other |
||||||||
Primary Insurance Carrier: _________________________ Type: |
Private Medicare |
Medicare Advantage |
Medicaid |
Tricare |
|||||||
Claims Submission Address: ________________________________________________________________________________________________
Subscriber ID/Policy Number: __________________ Group Number: ______________________ Plan: _______________________________
PATIENT AUTHORIZATIONS, ASSIGNMENT OF BENEFITS (AOB) & FINANCIAL RESPONSIBILITIES
I authorize Exact Sciences Laboratories (Exact) to bill my insurance/health plan and furnish them with my Cologuard order information, test results, or other information requested for reimbursement. I assign all rights and benefits under my insurance plans to Exact and authorize Exact to appeal and contest any reimbursement denial, including in any administrative or civil proceedings necessary to pursue reimbursement. I authorize all reimbursements to be paid directly to the laboratory in consideration for services performed. I understand that I am responsible for any amount not paid, including amounts for
Patient Signature: _________________________________________________________________ Date: ___________________
Fax completed form to
For Lab Use Only
Sample Collected: __ /__ /_____ Sample Received: __ /__ /_____
| Fact Name | Details |
|---|---|
| Company | Cologuard is provided by Exact Sciences Laboratories, LLC. |
| Test Type | This is a stool-based DNA test that includes a hemoglobin immunoassay component. |
| Provider Requirements | Healthcare providers must be licensed to order Cologuard and confirm the test's medical necessity. |
| Insurance Handling | Patients can choose to have Exact Sciences bill their insurance or pay out-of-pocket. |
| Patient Data Privacy | Exact Sciences is committed to maintaining patient privacy in accordance with HIPAA standards. |
| Sample Processing | Completed forms should be faxed to 844-870-8875 for further processing of the sample. |
Once you have received the Cologuard Order form, you will need to fill it out to initiate the testing process. This form captures essential information about the provider, patient demographics, and billing details. Follow the steps below carefully to complete the form.
What is the Cologuard Order form used for?
The Cologuard Order form is designed for healthcare providers to request the Cologuard test, which is a stool-based DNA test that helps screen for colorectal cancer. The test also includes a hemoglobin immunoassay component. This order form collects necessary provider and patient information to process the test accurately.
Who is eligible to complete the Cologuard Order form?
The form must be completed by a licensed healthcare provider who is authorized to order the Cologuard test. It is essential that the provider determine whether the test is appropriate for the specific patient based on their medical history and risk factors.
What information is required on the Cologuard Order form?
The form requires various details, including the healthcare organization name, provider name and NPI number, and patient demographics such as date of birth, sex, and contact information. Additionally, insurance details need to be provided if the patient wishes to have testing billed to their insurance carrier.
How should I submit the Cologuard Order form?
Completed Cologuard Order forms should be faxed to Exact Sciences Laboratories at 844-870-8875. It is important to ensure that all information is accurate to avoid delays in processing.
What are the patient's responsibilities regarding insurance and billing?
Patients must authorize Exact Sciences to bill their insurance for the test. They are responsible for any costs not covered by their plan, including potential out-of-pocket expenses. If the patient is a Medicaid enrollee, Exact will accept the Medicaid payments as full payment, along with any required deductibles or copayments.
How is patient privacy protected through the Cologuard Order form?
The provider signing the order form certifies that they will maintain the confidentiality of the patient's test results and related information in accordance with HIPAA regulations. This ensures that sensitive patient information is handled securely throughout the testing process.
Inconsistent Provider Information: Failing to provide complete and accurate information about the healthcare provider can lead to delays. Ensure the provider's name, organization, and contact details are correctly filled out.
Missing ICD-10 Codes: Not including the relevant diagnosis code(s) for the test may result in complications with insurance processing. Take care to select the appropriate codes, such as Z12.11 or Z12.12.
Invalid or Missing Signature: Forgetting to sign the order form or providing an illegible signature can delay the entire process. Remember that the signature is necessary to confirm authorization to order the Cologuard test.
Incomplete Patient Demographics: Provide full patient information, including date of birth and contact numbers. Leaving sections blank can hinder communication and processing.
Insurance Information Errors: Incorrect details in the insurance section, such as the policy number or insurance carrier, might lead to reimbursement complications. Double-check these details before submission.
Neglecting Patient Authentications: Overlooking the necessary patient authorizations and financial agreements might affect the billing process. Ensure all required authorizations are filled out accurately.
Along with the Cologuard Order form, several other forms and documents are commonly used in the process of testing and billing for Cologuard. Each document serves a specific purpose to ensure accurate communication and compliance with healthcare regulations.
Each of these documents plays a vital role in facilitating a smooth testing process and ensuring compliance with healthcare regulations. Having them completed accurately can help avoid delays in testing and billing, paving the way for timely patient care.
The Cologuard Order form shares similarities with a standard medical prescription form, which serves as a document that physicians provide to pharmacies to dispense medication. Both documents require identification of the healthcare provider and the patient, ensuring that essential details like names, addresses, and contact information are accurately filled out. Just like the Cologuard form, a medical prescription includes sections for the provider's signature and date, underscoring the importance of the medical professional's authorization for treatment. Additionally, both forms often have an insurance information section to facilitate potential reimbursement processes for the services rendered.
Another document closely related to the Cologuard Order form is a referral form used in healthcare settings when a patient needs to see a specialist. Referral forms, like the Cologuard form, are critical in outlining the patient's information and the specific services required. These forms usually include sections for the referring provider’s details and the reason for the referral, much like how the Cologuard form outlines the test being requested. Both documents help in ensuring that all necessary information flows smoothly between healthcare providers and that patient care is effectively coordinated.
The patient intake form is an additional document that relates to the Cologuard Order form. Both documents collect essential information about the patient, including demographics, insurance details, and medical history. Patient intake forms often request similar identifiers such as the patient's name, date of birth, and contact details. They also serve as a means of consent where required, just as the Cologuard form seeks the patient’s authorization for testing. By collecting this information upfront, both forms aim to streamline the process of patient care and ensure that healthcare providers have access to vital data.
Informed consent forms also share commonalities with the Cologuard Order form. Such forms are essential for detailing the procedure that a patient is about to undergo, including potential risks and benefits, thereby ensuring the patient is fully aware. Both types of forms require the patient’s signature to acknowledge understanding and agreement. While the Cologuard form focuses on approval for a specific test, informed consent forms might cover a broader range of medical procedures, yet both emphasize the necessity of transparency in the patient-provider relationship.
Lastly, the insurance claim form exhibits similarities with the Cologuard Order form, particularly in terms of processing payments for medical services. Both documents necessitate detailed information on the patient’s insurance provider, including policy numbers and the nature of the services rendered. The Cologuard form includes a section for the provider to authorize billing, which aligns with the purpose of an insurance claim form to seek reimbursement post-service. Both documents are essential in navigating the often-complex insurance landscape, ensuring that financial matters are addressed appropriately within the healthcare system.
When filling out the Cologuard Order form, there are important considerations to ensure accuracy and compliance. Below are ten do's and don'ts to guide you through the process.
Understanding the Cologuard order form can be challenging. Here are 10 common misconceptions about it, along with clarifications to help clear things up.
When filling out and using the Cologuard Order form, consider the following key takeaways: