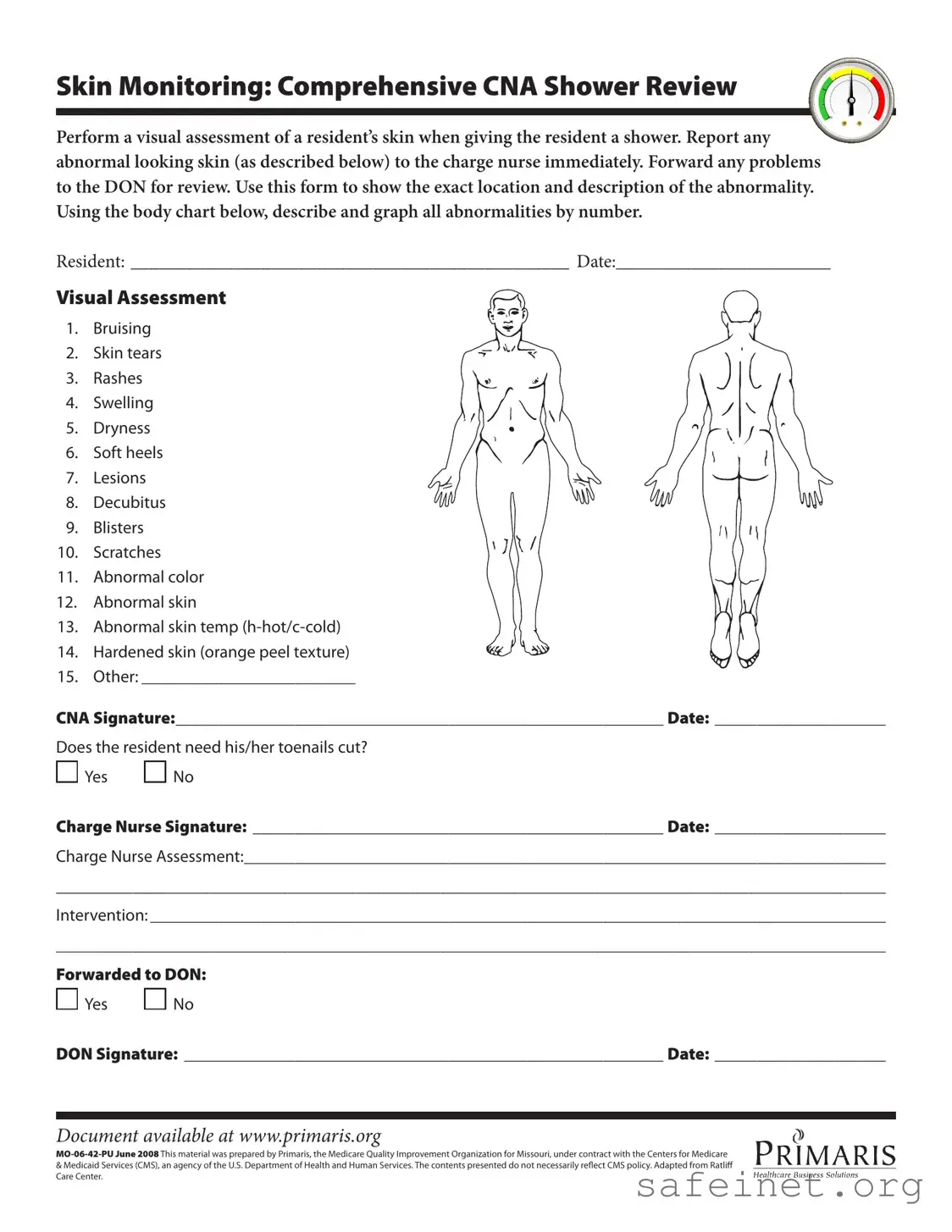
The CNA Shower Sheets form is a vital tool used in long-term care facilities to ensure the thorough monitoring of residents' skin health during showering. This form facilitates a systematic visual assessment, allowing Certified Nursing Assistants (CNAs) to document any abnormalities they observe, such as bruising, skin tears, rashes, or lesions. Each entry requires the CNA to specify the exact location of the issue on a body chart, thereby providing a clear visual representation of the resident's condition. Additionally, the form prompts CNAs to note other skin concerns, including dryness, swelling, and changes in skin temperature. Following the assessment, the CNA must report any findings to the charge nurse for immediate attention. The charge nurse then reviews the documentation, providing their signature and assessment, which may include recommendations for further intervention. If necessary, the issues are escalated to the Director of Nursing (DON) for additional review. The form also includes a section to determine if the resident requires toenail care, ensuring comprehensive personal hygiene is maintained. This structured approach not only promotes resident safety but also enhances communication among healthcare staff regarding skin health management.
| Fact Name | Description | Governing Law |
|---|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers, ensuring any abnormalities are reported promptly. | Federal regulations under 42 CFR Part 483, which govern nursing facility requirements. |
| Assessment Items | The form includes a list of 15 specific skin conditions to monitor, such as bruising, rashes, and lesions. | State-specific regulations may vary; refer to local health department guidelines. |
| Documentation | CNA signatures and charge nurse assessments are required, ensuring accountability and proper follow-up on any identified issues. | Applicable state nursing practice acts and regulations. |
| Forwarding Protocol | Any abnormalities must be forwarded to the Director of Nursing (DON) for further review and intervention. | Federal and state healthcare compliance laws. |
Completing the CNA Shower Sheets form is essential for documenting the visual assessment of a resident’s skin during their shower. This process ensures that any abnormalities are promptly reported and addressed. Follow the steps below to accurately fill out the form and maintain the highest standard of care for the residents.
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to help Certified Nursing Assistants (CNAs) conduct a thorough visual assessment of a resident’s skin during showering. This form enables CNAs to document any abnormalities, such as bruising, rashes, or lesions, and ensures that these findings are communicated to the charge nurse and the Director of Nursing (DON) for further evaluation. By using this form, CNAs play a crucial role in monitoring residents' skin health and preventing potential complications.
What types of skin abnormalities should I look for during the assessment?
During the shower assessment, CNAs should be vigilant for various skin abnormalities. Common issues to note include bruising, skin tears, rashes, swelling, dryness, and lesions. Additionally, pay attention to soft heels, decubitus ulcers, blisters, scratches, and any unusual skin color or temperature. Each of these conditions can indicate underlying health concerns that may require immediate attention. The form provides a body chart for CNAs to accurately mark and describe the location of these abnormalities.
What should I do if I find an abnormality on a resident's skin?
If you observe any abnormal skin conditions during the assessment, it is essential to report them to the charge nurse right away. The charge nurse will then evaluate the situation and decide on the necessary interventions. Afterward, the findings should be documented on the CNA Shower Sheets form, and any significant issues should be forwarded to the DON for further review. Prompt reporting helps ensure that residents receive the care they need in a timely manner.
How do I document my findings on the CNA Shower Sheets form?
To document your findings, start by filling out the resident's name and the date at the top of the form. As you conduct your visual assessment, use the provided body chart to graphically represent the location of any abnormalities. Next, describe each finding in the designated sections, noting the type of abnormality and any other relevant details. Don’t forget to sign and date the form after completing your assessment. Clear documentation is key to effective communication within the care team.
Is there anything else I need to do after completing the form?
Yes, after you complete the CNA Shower Sheets form, make sure to check if the resident needs their toenails cut, as indicated on the form. Once you have filled out all necessary sections, pass the form to the charge nurse for their assessment and signature. Finally, ensure that the form is forwarded to the DON if required. This process helps maintain a comprehensive record of the resident's skin health and ensures that all team members are informed of any concerns.
Neglecting to perform a visual assessment: One of the most critical steps is to conduct a thorough visual assessment of the resident’s skin during the shower. Skipping this step can lead to undetected issues.
Failing to report abnormalities: If any skin abnormalities are observed, it’s essential to report them to the charge nurse immediately. Delaying this can result in worsening conditions.
Inaccurate descriptions: When documenting abnormalities, providing vague or unclear descriptions can create confusion. It’s important to be specific about the location and nature of the issue.
Omitting the body chart: The body chart is a vital tool for mapping skin issues. Not using it to graph abnormalities can lead to miscommunication about the severity and location of the problems.
Ignoring the toenail assessment: The question regarding toenail care should not be overlooked. Neglecting to address this can affect the resident's overall hygiene and comfort.
Not obtaining necessary signatures: Failing to secure the charge nurse’s and DON’s signatures can lead to incomplete documentation, which may have repercussions for care continuity.
Forgetting to document interventions: It’s crucial to record any interventions taken after the assessment. This documentation is essential for tracking the resident’s care and progress.
The CNA Shower Sheets form plays a crucial role in monitoring residents' skin health during showers. However, several other forms and documents complement this process, ensuring a comprehensive approach to care. Below are some commonly used documents that work alongside the CNA Shower Sheets form.
Each of these documents plays a vital role in ensuring that residents receive the highest standard of care. By working in tandem with the CNA Shower Sheets form, they create a holistic approach to health monitoring and intervention.
The CNA Shower Sheets form serves a vital role in monitoring resident health during bathing. It bears similarities to the Incident Report form, which documents any unusual occurrences or accidents involving residents. Both documents require immediate reporting to a supervising nurse, ensuring timely attention to potential health issues. The emphasis on thoroughness in both forms helps maintain a high standard of care and accountability in healthcare settings.
Another document akin to the CNA Shower Sheets is the Skin Assessment Form. This form specifically focuses on the evaluation of skin conditions, much like the shower sheets do during bathing. Both forms necessitate a visual examination and require detailed descriptions of any abnormalities found. This similarity aids in tracking skin health over time, allowing for prompt interventions when necessary.
The Care Plan Review is another relevant document. It outlines the individualized care strategies for residents, including skin care protocols. Just as the CNA Shower Sheets document specific observations during showers, the Care Plan Review ensures that all healthcare providers are aware of and follow the established guidelines for each resident's unique needs. This consistency promotes better health outcomes.
Similar to the CNA Shower Sheets is the Daily Nursing Log. This log records daily observations and activities related to resident care. Both documents facilitate communication among nursing staff, ensuring that important information about a resident's condition is shared. The Daily Nursing Log, like the shower sheets, is crucial for maintaining continuity of care.
The Medication Administration Record (MAR) also shares similarities with the CNA Shower Sheets. Both documents require precise documentation regarding resident care. While the MAR focuses on medication given, the shower sheets emphasize skin assessments during bathing. Each document plays a key role in ensuring that all aspects of a resident's health are monitored and managed effectively.
The Resident Assessment Protocol (RAP) is another document that aligns with the CNA Shower Sheets. RAPs provide a structured approach to evaluating various health aspects of residents, including skin integrity. Both documents highlight the importance of thorough assessments and timely reporting, which are essential for preventing complications and ensuring optimal care.
In addition, the Falls Risk Assessment form is relevant. It evaluates a resident's risk of falling, similar to how the CNA Shower Sheets assess skin integrity during showers. Both documents require healthcare providers to identify potential issues and implement preventative measures. This proactive approach helps safeguard residents from injuries and promotes their overall well-being.
The Vital Signs Record also bears resemblance to the CNA Shower Sheets. While the former focuses on tracking vital signs, the latter emphasizes skin condition during bathing. Both documents require consistent monitoring and documentation, which is essential for identifying changes in a resident's health status. This vigilance is crucial in delivering effective care.
Lastly, the Incident Follow-Up form complements the CNA Shower Sheets. After any incident, this form captures the actions taken and the outcomes. Like the shower sheets, it emphasizes the need for prompt reporting and intervention. Both documents are vital for ensuring that all aspects of resident care are addressed and that any issues are resolved swiftly.
When filling out the CNA Shower Sheets form, it's essential to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn't do:
By adhering to these guidelines, you contribute to the resident's care and ensure proper documentation for future reference.
Misconceptions about the CNA Shower Sheets form can lead to confusion and improper care. Here are six common misunderstandings:
Understanding these misconceptions is vital for providing the best care possible. Accurate documentation and communication can significantly impact resident health outcomes.
Here are some key takeaways about filling out and using the CNA Shower Sheets form: