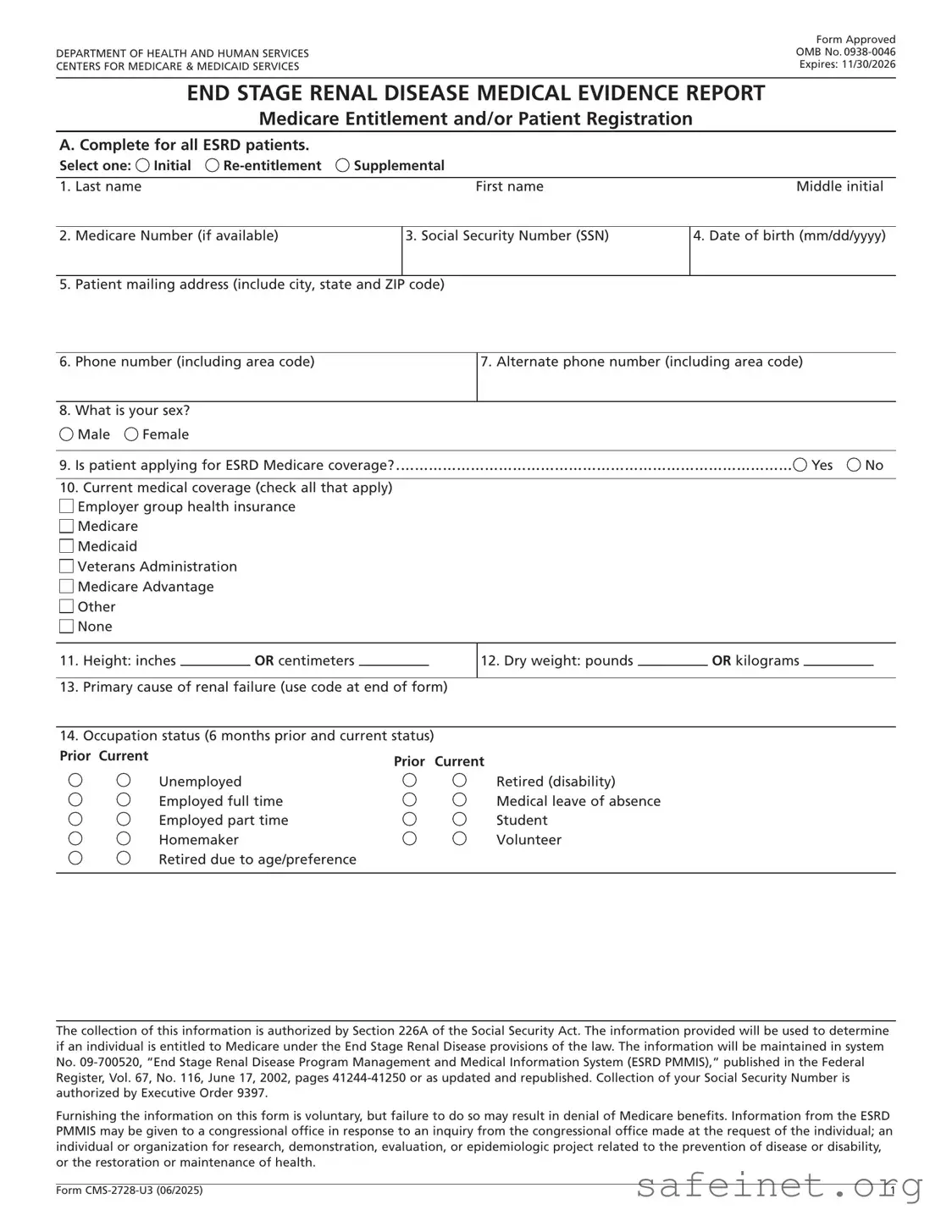
The CMS 2728 U3 form plays a crucial role in the healthcare system, particularly for patients facing end-stage renal disease (ESRD). This form is essential for establishing Medicare entitlement and patient registration, making it a key document for both patients and healthcare providers. It must be completed for all ESRD patients, whether they are new applicants or those seeking re-entitlement or supplemental benefits. The form collects vital information, including the patient’s name, Medicare Beneficiary Identifier, date of birth, and medical history. Additionally, it requires details about the patient's current medical coverage, height, weight, and primary cause of renal failure, which helps in determining eligibility for Medicare benefits. The CMS 2728 U3 also addresses the patient's employment status, co-morbid conditions, and prior treatments, ensuring a comprehensive overview of their health status. This thorough documentation is not only a requirement for Medicare but also a means to facilitate better care and support for patients navigating the complexities of ESRD treatment options.



| Fact Name | Fact Description |
|---|---|
| Purpose | The CMS 2728 U3 form is used to report medical evidence for patients with End Stage Renal Disease (ESRD) seeking Medicare benefits. |
| Submission Timeline | This form must be completed within 45 days of the patient's first dialysis treatment or kidney transplant. |
| Patient Information | It collects essential details such as the patient's name, Medicare Beneficiary Identifier, date of birth, and contact information. |
| Co-Morbid Conditions | The form includes a section to check for co-morbid conditions that may affect the patient's treatment. |
| Types of Dialysis | It allows patients to specify their primary type of dialysis, whether it's home dialysis or facility-based. |
| Governing Law | This form is governed by the Social Security Act and related Medicare regulations. |
| Privacy Statement | The form includes a privacy statement outlining how the collected information will be used and protected. |
| Signature Requirement | Both the patient and the attending physician must sign the form to verify the information provided. |
Completing the CMS 2728 U3 form is a necessary step for patients seeking Medicare coverage due to end-stage renal disease. This form gathers essential information about the patient’s medical history, treatment, and current status. Following these steps will ensure that the form is filled out accurately and completely.
What is the CMS 2728 U3 form?
The CMS 2728 U3 form is a medical evidence report used to determine Medicare entitlement for patients with End Stage Renal Disease (ESRD). It collects essential patient information, including demographics, medical history, and treatment details, to assess eligibility for Medicare benefits related to kidney disease treatment.
Who needs to complete the CMS 2728 U3 form?
This form must be completed for all patients diagnosed with ESRD who are beginning dialysis treatment or are receiving a kidney transplant. It should not be completed for patients in acute renal failure, as their condition is expected to improve.
What information is required on the CMS 2728 U3 form?
The form requires various details, including the patient’s name, Medicare Beneficiary Identifier or Social Security Number, date of birth, mailing address, phone number, sex, ethnicity, and race. Additionally, it collects medical coverage information, height, weight, primary cause of renal failure, employment status, and any co-morbid conditions.
How is the primary cause of renal failure determined on the form?
The attending physician is responsible for identifying the primary cause of renal failure using a list of ICD-10 codes provided on the form. If multiple causes are present, the physician should select the most significant one as the primary cause.
What are the categories for submitting the CMS 2728 U3 form?
The form can be submitted under three categories: Initial, for patients starting dialysis or receiving a transplant; Re-entitlement, for patients returning to dialysis after a break; and Supplemental, for patients who have received a transplant or completed self-care dialysis training shortly after the initial submission.
What happens if the form is not completed within the required timeframe?
The CMS 2728 U3 form must be completed within 45 days of the patient's initiation of dialysis or transplant. Failure to submit the form on time may result in delays or denial of Medicare benefits for the patient.
What is the role of the attending physician in completing the form?
The attending physician must provide accurate medical information and certify the patient's condition on the form. They are responsible for completing specific sections, including the primary cause of renal failure and co-morbid conditions, and must sign the attestation to confirm the information's accuracy.
How does a patient authorize the release of their medical information?
Patients must sign the authorization section of the CMS 2728 U3 form, allowing their medical records to be disclosed to the Department of Health and Human Services. This authorization is necessary for reviewing their application for Medicare entitlement.
What should patients do with the completed form?
Once completed, the form should be submitted to the Social Security office servicing the claim. A copy should also be maintained by the dialysis facility or healthcare provider involved in the patient's treatment.
Incomplete Patient Information: Failing to provide all required personal details, such as the patient's full name, date of birth, and Medicare Beneficiary Identifier, can lead to delays in processing the application.
Incorrect Coding: Using the wrong ICD-10-CM code for the primary cause of renal failure can result in incorrect classification and potential denial of Medicare benefits.
Missing Signatures: Not obtaining necessary signatures from the patient and the attending physician can invalidate the form. Ensure all required signatures are present before submission.
Omitting Medical History: Failing to accurately report the patient's medical history, including co-morbid conditions and previous treatments, may affect eligibility for Medicare coverage.
Incorrect Dates: Providing incorrect dates for dialysis treatment or transplant can cause confusion and may lead to delays in processing the application.
Not Checking Eligibility: Not verifying whether the patient is eligible for ESRD Medicare coverage before completing the form can result in unnecessary applications and wasted time.
Failure to Follow Instructions: Ignoring specific instructions regarding which items must be completed by the physician or other healthcare providers can lead to incomplete submissions.
The CMS 2728 U3 form is essential for patients with End Stage Renal Disease (ESRD) seeking Medicare benefits. Alongside this form, several other documents may be required to support the application process. Below is a list of documents that are often used in conjunction with the CMS 2728 U3 form.
These documents collectively support the application process for Medicare benefits related to ESRD. Ensuring all necessary forms are completed accurately and submitted in a timely manner can help facilitate a smoother approval process for patients in need of assistance.
The CMS 2728 U3 form is akin to the CMS 1500 form, which is used for billing Medicare and Medicaid for outpatient services. Both documents require detailed patient information and medical history, ensuring that healthcare providers can accurately represent services rendered. The CMS 1500 focuses more on the billing aspect, while the CMS 2728 U3 emphasizes medical evidence related to end-stage renal disease (ESRD). Each form serves a specific purpose but shares the goal of facilitating patient care and coverage under Medicare.
Another document similar to the CMS 2728 U3 is the Medicare Enrollment Application (CMS-10106). This form is essential for individuals seeking to enroll in Medicare, capturing personal details, eligibility, and coverage choices. Like the CMS 2728 U3, it requires accurate patient information to ensure that Medicare can effectively process and approve coverage. Both forms play crucial roles in the enrollment process, with the CMS 2728 U3 specifically addressing the needs of ESRD patients.
The Health Insurance Claim Form (UB-04) also shares similarities with the CMS 2728 U3. Used primarily by hospitals and facilities, the UB-04 captures information necessary for billing Medicare and other insurers. Both forms require comprehensive patient details and medical history to validate claims. While the UB-04 focuses on facility-based services, the CMS 2728 U3 is tailored for patients with renal disease, highlighting their specific medical needs.
Additionally, the CMS 64 form, used for reporting Medicaid expenditures, is another document that parallels the CMS 2728 U3. Both forms require detailed financial and patient information to ensure proper reimbursement for services. The CMS 64 focuses on state Medicaid programs, while the CMS 2728 U3 is specific to Medicare coverage for ESRD patients. Each form is crucial in maintaining the integrity of healthcare funding and patient care.
The Patient Registration Form is also similar to the CMS 2728 U3. This document collects essential information about patients before they receive care. It captures personal details, medical history, and insurance information, much like the CMS 2728 U3, which is specifically designed for patients with ESRD. Both forms ensure that healthcare providers have the necessary information to deliver appropriate care and submit accurate claims.
Lastly, the Advance Beneficiary Notice of Noncoverage (ABN) is related to the CMS 2728 U3 in that both address Medicare coverage. The ABN informs patients when a service may not be covered by Medicare, while the CMS 2728 U3 establishes entitlement to Medicare benefits for ESRD patients. Both forms require clear communication about patient rights and responsibilities, ensuring that patients are informed about their coverage status and potential costs.
When filling out the CMS 2728 U3 form, it's essential to follow certain guidelines to ensure accuracy and compliance. Here’s a list of things you should and shouldn’t do:
Following these guidelines can help streamline the application process for Medicare entitlement under the End Stage Renal Disease provisions. Accuracy is crucial, so take your time and double-check all entries before submission.
Here are five common misconceptions about the CMS 2728 U3 form:
This form is required for all patients with end-stage renal disease (ESRD), including those who have received a kidney transplant or are in the process of self-dialysis training.
In fact, the CMS 2728 U3 form must be completed for all ESRD patients within 45 days of starting dialysis or receiving a transplant. It is essential for establishing Medicare entitlement.
While the attending physician must complete specific sections, other healthcare professionals, such as head nurses or social workers, can also assist in filling out the form.
Although the form is primarily used for Medicare entitlement, it applies to all ESRD patients, regardless of their current insurance status. It helps document their medical condition and treatment needs.
The CMS 2728 U3 form contains sensitive medical information. It is protected under privacy regulations, and the information is used solely for the purpose of determining Medicare eligibility and related healthcare needs.
When filling out the CMS 2728 U3 form, it's essential to ensure accuracy and completeness. Here are some key takeaways: