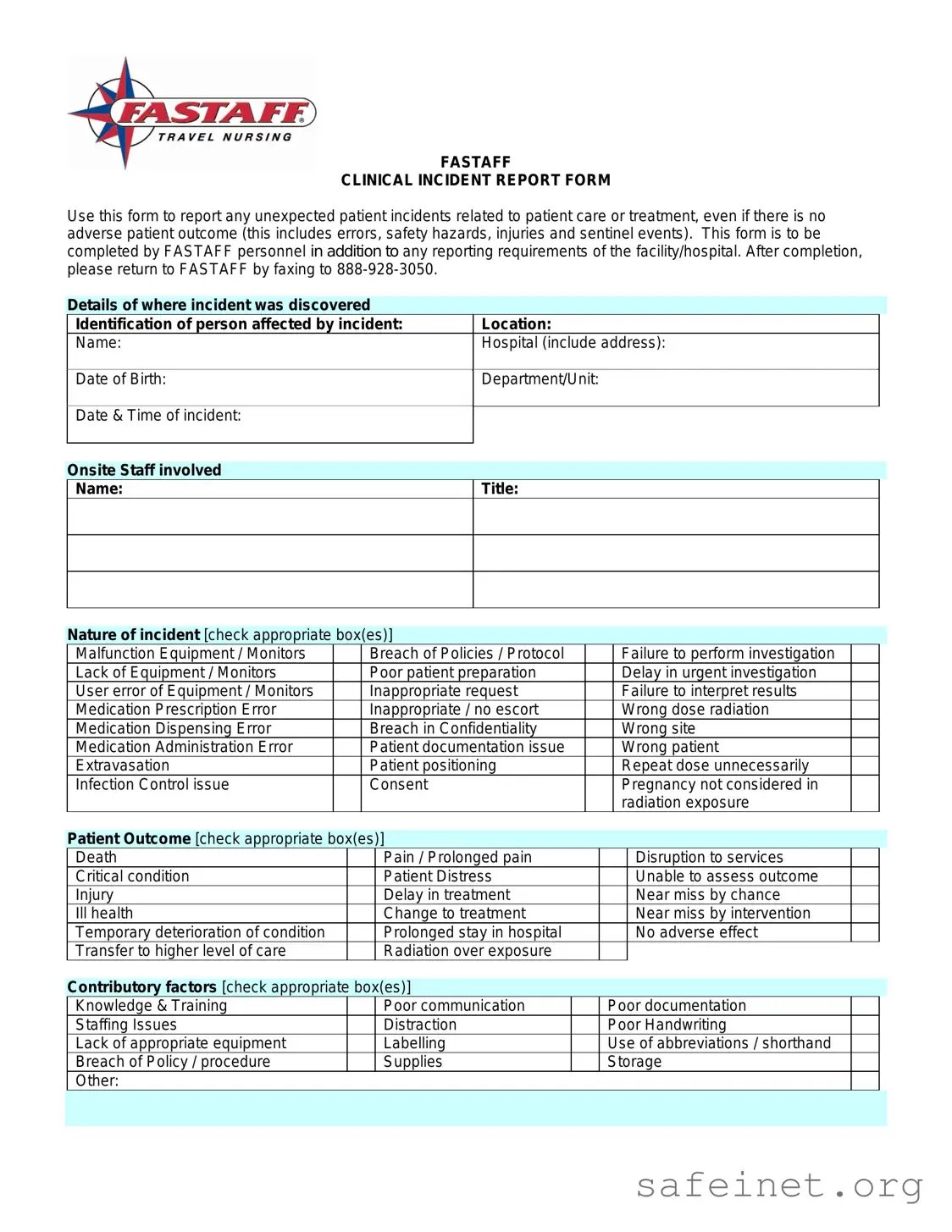
The Clinical Incident Report Sample form serves as an essential tool for documenting unexpected incidents that occur during patient care or treatment. This form is designed to capture a wide range of incidents, including errors, safety hazards, and even sentinel events, regardless of whether there was an adverse outcome for the patient. It must be filled out by FASTAFF personnel and submitted in conjunction with any additional reporting requirements set by the facility or hospital. Key sections of the form include details about the incident's location, the identification of the affected person, and the names and titles of involved onsite staff. Users are prompted to check appropriate boxes to categorize the nature of the incident, such as equipment malfunction, medication errors, or breaches of policy. The form also requests information about the patient outcome and any contributory factors that may have played a role in the incident. A summary section allows for a factual recounting of events, while a space for action taken ensures that necessary steps for treatment and prevention are documented. Finally, employee acknowledgment is required to confirm the accuracy of the information provided, and internal use sections allow for further action by FASTAFF’s Director of Credentialing.
| Fact Name | Description |
|---|---|
| Purpose | This form is designed to report unexpected patient incidents related to care or treatment, regardless of whether there was an adverse outcome. |
| Completion Requirement | FASTAFF personnel must complete the form in addition to any reporting requirements of the facility or hospital involved. |
| Submission Method | Once filled out, the form should be faxed to FASTAFF at 888-928-3050. |
| Incident Categories | Incidents can include equipment malfunctions, policy breaches, user errors, and medication errors, among others. |
| Patient Outcome Options | Outcomes can range from death and critical condition to no adverse effect or temporary deterioration. |
| Governing Laws | State-specific laws may apply; for example, in California, the reporting is governed by the California Health and Safety Code. |
Completing the Clinical Incident Report Sample form is a crucial step in documenting unexpected patient incidents. Accurate and thorough information is essential for ensuring patient safety and improving care protocols. Follow these steps carefully to fill out the form correctly.
After filling out the form, ensure it is returned to FASTAFF by faxing it to 888-928-3050. This step is vital for maintaining accurate records and facilitating further investigation if necessary.
What is the purpose of the Clinical Incident Report Sample form?
The Clinical Incident Report Sample form is designed to document any unexpected incidents related to patient care or treatment. This includes errors, safety hazards, injuries, and sentinel events, regardless of whether there was an adverse outcome for the patient. It serves as a tool for FASTAFF personnel to report these incidents while also fulfilling any additional reporting requirements of the facility or hospital.
Who should complete the Clinical Incident Report?
The form should be completed by FASTAFF personnel involved in the incident. It is crucial that the person filling out the form provides accurate and factual information about the incident to ensure proper documentation and follow-up actions.
What information is required on the form?
The form requires various details, including the identification of the person affected by the incident, the location and date of the incident, the names and titles of onsite staff involved, and a description of the nature of the incident. Additionally, it asks for a summary of what happened, any actions taken as a result, and the acknowledgment of the employee involved.
What should be included in the summary of what happened?
The summary should focus solely on the facts of the incident without including personal opinions. If more space is needed, it is acceptable to attach a separate sheet. This factual account helps maintain clarity and objectivity in the reporting process.
What actions should be taken after an incident is reported?
After completing the report, it is essential to ensure that all necessary steps have been taken to support and treat anyone injured. Additionally, measures should be implemented to prevent further incidents. Keeping medical records factual and up to date is also a critical part of the process.
How should the form be submitted after completion?
Once the form is completed, it should be returned to FASTAFF by faxing it to 888-928-3050. Timely submission is important to ensure that the incident is addressed appropriately and any necessary follow-up actions can be taken.
What happens to the report after it is submitted?
After submission, the report will be reviewed by the FASTAFF Director of Credentialing, who will document any actions taken as a result of the incident. This internal review process helps ensure accountability and continuous improvement in patient care practices.
What if I have more questions about the form or the reporting process?
If you have additional questions or need further clarification about the Clinical Incident Report Sample form or the reporting process, it is advisable to reach out to your supervisor or the FASTAFF administrative office. They can provide guidance and support to ensure compliance with reporting requirements.
Incomplete Information: Failing to provide all necessary details, such as the patient's name, date of birth, or the exact location of the incident, can lead to confusion and delays in addressing the situation.
Omitting Witnesses: Not including the names and titles of onsite staff involved in the incident may hinder investigations and accountability.
Insufficient Description: Providing vague or unclear summaries of what happened can result in misunderstandings about the nature of the incident.
Failure to Check Appropriate Boxes: Neglecting to mark all relevant boxes for the nature of the incident or patient outcome may lead to an incomplete assessment of the situation.
Ignoring Follow-Up Actions: Not detailing the actions taken as a result of the incident can prevent proper resolution and future prevention strategies.
Using Abbreviations or Shorthand: Utilizing abbreviations may create confusion for those reviewing the report, as not everyone may understand the shorthand used.
Submitting Without Review: Failing to review the report for accuracy before submission can lead to the dissemination of incorrect information.
Neglecting Confidentiality: Sharing sensitive information about the incident without proper consideration of confidentiality can violate privacy regulations.
Not Following Facility Protocols: Ignoring additional reporting requirements set by the facility or hospital can result in non-compliance and potential repercussions.
The Clinical Incident Report Sample form serves as a critical tool for documenting unexpected patient incidents. However, several other forms and documents are often utilized alongside it to ensure comprehensive reporting and management of incidents. Below is a list of these related documents, each serving a specific purpose in the incident reporting process.
Utilizing these forms and documents in conjunction with the Clinical Incident Report Sample form enhances the ability to track, analyze, and improve patient safety and care quality. Together, they create a comprehensive framework for managing incidents effectively within healthcare settings.
The Incident Report Form serves as a crucial tool in healthcare settings, similar to the Patient Safety Report. Both documents aim to identify and document incidents that may compromise patient safety. The Patient Safety Report focuses on the systemic issues that lead to adverse events, encouraging a culture of safety and transparency. It typically includes sections for describing the event, identifying contributing factors, and outlining corrective actions. While the Clinical Incident Report Sample form addresses individual incidents, the Patient Safety Report takes a broader view, promoting learning and improvement within the healthcare system.
Another document akin to the Clinical Incident Report is the Adverse Event Report. This report specifically captures events that result in harm to a patient, whether the harm is physical, emotional, or psychological. Like the Clinical Incident Report, it seeks to document the specifics of the incident, including the nature of the event and the individuals involved. However, the Adverse Event Report often emphasizes the outcomes of the incident more heavily, focusing on the impact on the patient and the necessary follow-up actions to mitigate future risks.
The Root Cause Analysis (RCA) report is also similar in purpose, as it investigates the underlying factors contributing to incidents. While the Clinical Incident Report provides a snapshot of an incident, the RCA delves deeper, analyzing the sequence of events and identifying systemic weaknesses. The RCA report typically includes recommendations for changes in policies or procedures to prevent recurrence. Both documents share the goal of enhancing patient safety, but the RCA is more comprehensive in its approach to understanding the causes of incidents.
The Risk Management Report parallels the Clinical Incident Report in its focus on identifying and mitigating risks within a healthcare environment. This report often aggregates data from various incidents, including those documented in Clinical Incident Reports, to identify trends and areas for improvement. It serves as a tool for healthcare administrators to make informed decisions about resource allocation and policy changes, ultimately aiming to reduce the likelihood of future incidents. Both reports emphasize the importance of documentation and follow-up actions to improve patient care.
The Medication Error Report is another document that aligns closely with the Clinical Incident Report. It specifically targets errors related to medication administration, including incorrect dosages, wrong medications, or failure to administer medication altogether. Like the Clinical Incident Report, it requires detailed documentation of the incident, including the context and any contributing factors. This report aims to enhance medication safety by identifying patterns and implementing corrective measures to prevent future errors.
The Safety Hazard Report is similar in that it addresses potential risks that could lead to incidents. This document focuses on identifying hazards within the healthcare environment, such as unsafe equipment or environmental risks. While the Clinical Incident Report deals with incidents that have already occurred, the Safety Hazard Report aims to proactively identify and mitigate risks before they result in harm. Both documents play a vital role in fostering a culture of safety and accountability in healthcare settings.
The Incident Action Plan is another relevant document, as it outlines the immediate steps to be taken following an incident. While the Clinical Incident Report captures the details of the incident itself, the Incident Action Plan focuses on the response and management of the situation. It includes specific actions to address the incident, support affected individuals, and prevent future occurrences. Both documents are essential for ensuring that incidents are managed effectively and that lessons are learned for future improvement.
Finally, the Compliance Report shares similarities with the Clinical Incident Report in its focus on adherence to established protocols and regulations. This report often highlights incidents where compliance has been breached, leading to potential risks for patients. While the Clinical Incident Report documents specific incidents, the Compliance Report takes a broader view, assessing overall adherence to safety standards and regulatory requirements. Both documents are integral to maintaining high standards of care and ensuring patient safety within healthcare organizations.
When filling out the Clinical Incident Report Sample form, it is essential to approach the task with care and attention to detail. Below are five important guidelines to consider:
By following these guidelines, you can contribute to a thorough and effective reporting process, ultimately enhancing patient safety and care.
Misconceptions about the Clinical Incident Report Sample form can lead to misunderstandings about its purpose and use. Here are four common misconceptions:
Here are key takeaways for filling out and using the Clinical Incident Report Sample form: