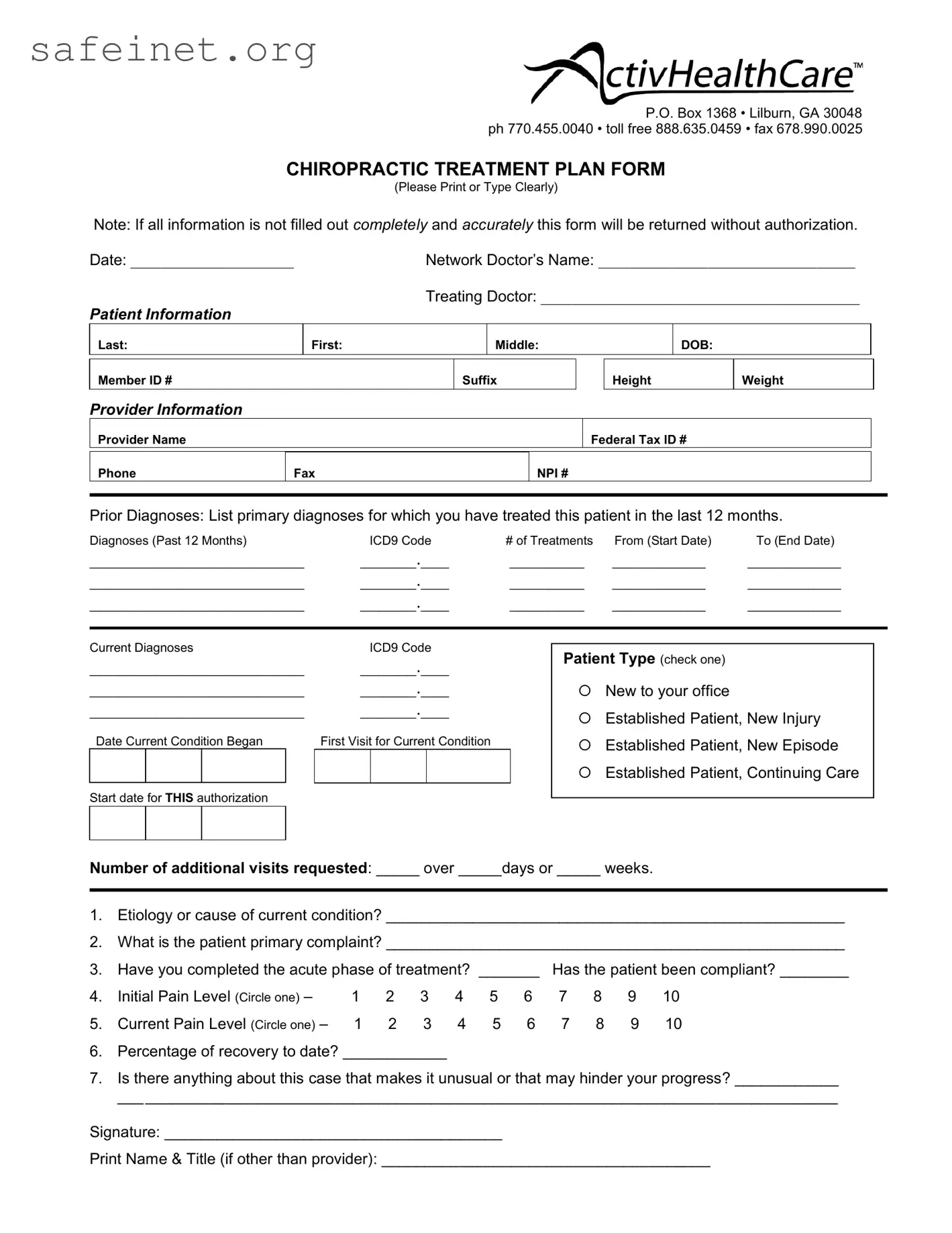
The Chiropractic Treatment Plan form plays a crucial role in ensuring effective communication between healthcare providers and patients. This form collects essential patient information, including contact details and medical history, which serves as a foundation for treatment planning. When filling out the form, patients will identify their current and prior diagnoses, complete with corresponding ICD9 codes, underscoring the importance of precise medical documentation. It also highlights the relationship between the patient and the provider, indicating if the patient is new or established, as well as detailing the treatment history over the past year. Specific sections focus on the patient’s condition, including the etiology of their issues and any noted compliance with prior treatments. Pain levels both at the beginning and during the current treatment phases are documented, offering vital insights into the patient's recovery journey. Understanding the percentage of recovery and any unusual case characteristics can further guide the treatment approach. All this information is essential not only for facilitating proper care but also for the authorization process. Accuracy is paramount—any incomplete or inaccurate submissions may be returned without authorization, emphasizing the need for thoroughness in this critical documentation.
P.O. Box 1368 • Lilburn, GA 30048 ph 770.455.0040 • toll free 888.635.0459 • fax 678.990.0025
CHIROPRACTIC TREATMENT PLAN FORM
(Please Print or Type Clearly)
Note: If all information is not filled out completely and accurately this form will be returned without authorization.
Date: _____________________
PATIENT INFORMATION
Last:
Network Doctor’s Name: _________________________________
Treating Doctor: _________________________________________
First: |
Middle: |
DOB: |
|
|
|
Member ID #
Suffix
Height
Weight
PROVIDER INFORMATION
Provider Name
Federal Tax ID #
Phone
Fax
NPI #
Prior Diagnoses: List primary diagnoses for which you have treated this patient in the last 12 months.
Diagnoses (Past 12 Months) |
ICD9 Code |
# of Treatments |
From (Start Date) |
To (End Date) |
||||||
_______________________ |
______.___ |
________ |
__________ |
__________ |
||||||
_______________________ |
______.___ |
________ |
__________ |
__________ |
||||||
_______________________ |
______.___ |
________ |
__________ |
__________ |
||||||
|
|
|
|
|
|
|||||
Current Diagnoses |
ICD9 Code |
|
Patient Type (check one) |
|
||||||
_______________________ |
______.___ |
|
|
|||||||
|
|
|
|
|||||||
_______________________ |
______.___ |
|
New to your office |
|
||||||
_______________________ |
______.___ |
|
Established Patient, New Injury |
|||||||
|
|
|
|
|
|
|
|
|||
Date Current Condition Began |
First Visit for Current Condition |
|
Established Patient, New Episode |
|||||||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Established Patient, Continuing Care |
||
Start date for THIS authorization |
|
|
|
|
|
|
|
|||
|
|
|
|
|
||||||
Number of additional visits requested: _____ over _____days or _____ weeks. |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
1.Etiology or cause of current condition? _____________________________________________________
2.What is the patient primary complaint? _____________________________________________________
3. |
Have you completed the acute phase of treatment? _______ |
Has the patient been compliant? ________ |
|||||||||
4. |
Initial Pain Level (Circle one) – |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
5. |
Current Pain Level (Circle one) – |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
6.Percentage of recovery to date? ____________
7.Is there anything about this case that makes it unusual or that may hinder your progress? ____________
___________________________________________________________________________________
Signature: _______________________________________
Print Name & Title (if other than provider): ______________________________________
| Fact Name | Details |
|---|---|
| Form Purpose | This form is designed to outline the chiropractic treatment plan for a patient, ensuring that all necessary information is provided to facilitate authorization for treatment. |
| Patient Information | It is essential for the patient’s demographic details, including name and date of birth, to be filled in clearly to avoid processing delays. |
| Diagnosis Reporting | Providers must list all past and current diagnoses, complete with ICD9 codes, to accurately reflect the patient’s medical history and treatment needs. |
| Compliance Confirmation | The form requires information on whether the patient has been compliant with their treatment plan, which is vital for continuity of care. |
| Pain Level Assessment | Patients must indicate their initial and current pain levels on a scale from 1 to 10, providing a quick assessment of their progress. |
| Authorization Timeframe | Providers can request a specific number of additional visits within a defined period, which helps manage the treatment timeline and patient expectations. |
| Georgia Law Reference | This form adheres to the regulations under Georgia law regarding chiropractic care documentation, ensuring compliance with the state's healthcare standards. |
Completing the Chiropractic Treatment Plan form is essential for ensuring accurate patient records and authorization for treatment. Follow the steps below to fill out the form completely and correctly.
What is the purpose of the Chiropractic Treatment Plan form?
This form serves as a vital tool for documenting patient information and treatment details. It ensures that all necessary data is collected for authorization purposes, allowing healthcare providers to outline the course of treatment effectively. Accurate and complete information helps in both managing patient care and facilitating insurance claims.
What information do I need to provide about myself?
Patients must provide several key details. This includes your last name, first name, middle initial, date of birth, and member ID. Additionally, it's important to include your height and weight. Providing accurate personal information is essential for establishing a clear treatment plan tailored to your needs.
Who should fill out the provider information section?
The healthcare provider responsible for your treatment should complete the provider information section. This includes writing the name of the provider, their federal tax ID number, and contact details. Ensuring this section is filled out correctly aids in identifying the submitting provider for any future correspondence or clarifications.
What are prior diagnoses, and why do they matter?
Prior diagnoses refer to the primary conditions for which the patient received treatment in the past year. Listing this information is crucial, as it helps the current provider understand your medical history and make informed decisions about ongoing treatment plans. Accurate documentation of past diagnoses also supports insurance claims and necessitates better continuity of care.
What does the section on current diagnoses require?
The current diagnoses section requires providers to specify any diagnoses relevant to your present condition. Each diagnosis must be linked to an ICD9 code, providing a standardized way of identifying the condition. This information is essential for both clinical assessment and insurance purposes.
What is the significance of the patient type options?
Defining your patient type is important for the treatment provider. It indicates whether you are new to the office, an established patient with a new injury, or continuing care for a prior condition. This classification influences the treatment strategy and the number of visits authorized for submittal.
Why do I need to indicate the number of additional visits requested?
Indicating the number of additional visits needed and the timeframe for those visits is crucial for obtaining authorization from insurance. It allows the provider to justify ongoing treatment and helps manage your care plan effectively. Without this information, the form may be returned for further clarification.
What do the pain level options mean?
Patients are asked to rate their initial and current pain levels on a scale of 1 to 10. This subjective measure helps healthcare providers gauge the severity of your condition and assess progress throughout treatment. Tracking changes in pain levels can inform necessary adjustments to your therapy.
What should I discuss if there is something unusual about my case?
If you have any concerns that might affect your treatment progress, it is essential to communicate these clearly in the provided section. This could include underlying health issues, specific challenges in recovery, or unique medical concerns. Sharing this information allows the provider to better tailor the treatment plan to suit your individual circumstances.
What should I do after completing the Chiropractic Treatment Plan form?
Once the form is complete, it needs to be signed by the treating doctor or authorized representative. Ensure all fields are filled out accurately before submission. Incomplete forms may be returned for clarification, causing delays in the authorization process. Keep a copy of the completed form for your records as well.
Insufficient Patient Information: Failing to fully complete patient details, such as last name, first name, middle name, or date of birth can lead to processing delays.
Inaccurate Diagnoses: Not providing correct or complete primary and current diagnoses will cause problems. Double-check ICD9 codes to ensure they match the conditions treated.
Missing Treatment Dates: Omitting the start and end dates for treatments can create confusion regarding the timeline of care.
Patient Type Selection: Not checking the correct patient type (new patient, established with new injury, etc.) may lead to authorization issues.
Unclear Primary Complaint: Writing vague descriptions for the patient's primary complaint fails to convey important information. Be specific.
Compliance Status Not Indicated: Forgetting to confirm whether the patient has completed the acute phase and has been compliant may affect approval for further treatment.
Inaccurate Pain Levels: Not accurately circling the pain levels, either initial or current, can weaken the representation of the patient’s condition.
Overlooking Special Case Notes: Leaving the section on unusual case factors blank means potentially important information is lost.
In addition to the Chiropractic Treatment Plan form, several other documents are commonly used in the chiropractic care process. Each serves a specific purpose to ensure that patient care is thorough and well-documented.
These documents work together to enhance patient care and create a comprehensive record for both healthcare providers and patients. Accurate and complete documentation supports better treatment outcomes and facilitates effective communication among all parties involved.
The Chiropractic Treatment Plan form shares similarities with the Medical History Form. Both documents collect essential patient details, including personal information and treatment history. While the Chiropractic Treatment Plan focuses on diagnosing and outlining future treatments, the Medical History Form gathers comprehensive past medical data. Each aims to ensure that healthcare providers understand a patient’s background and current health status, facilitating informed decision-making in the treatment process.
Another similar document is the Patient Intake Form, which serves as an initial assessment tool in healthcare settings. The Patient Intake Form gathers pertinent information about the patient's medical background, current symptoms, and lifestyle factors. Like the Chiropractic Treatment Plan, it is designed to provide insights that help healthcare providers tailor their approach. By ensuring complete and accurate information, providers can deliver effective and personalized care to their patients.
The Progress Note is also closely related to the Chiropractic Treatment Plan. This document is used regularly to record updates on a patient’s condition and response to treatment over time. Just as the Treatment Plan outlines expected treatments, Progress Notes reflect ongoing patient assessments, adherence to the plan, and changes in treatment as necessary. Together, these documents create a comprehensive view of the patient's journey through care.
In addition, the Consent to Treat Form plays a crucial role in the treatment process. This document authorizes healthcare providers to perform necessary procedures after informing the patient about potential risks and benefits. While the Chiropractic Treatment Plan details what treatments will be undertaken, the Consent to Treat Form confirms the patient's understanding and agreement, thereby enhancing communication and trust between the patient and provider.
The Referral Letter is another document that parallels the Chiropractic Treatment Plan. This letter is issued when a healthcare provider refers a patient to a specialist for further evaluation or treatment. Similar to the Treatment Plan, it details the patient's conditions and the rationale for referral. Both documents aim to maintain continuity of care and ensure that all relevant information is shared to facilitate effective treatment.
The SOAP Note is also akin to the Chiropractic Treatment Plan. SOAP stands for Subjective, Objective, Assessment, and Plan, and this structure helps document patient visits in a systematic way. While the Treatment Plan outlines intended future interventions, the SOAP Note reflects patient visits and highlights crucial updates, including the effectiveness of ongoing treatments and any adjustments required, providing a dynamic view of patient care.
Further, the Authorization for Treatment document is another important element in a patient’s care pathway. This document seeks consent for specific treatments based on the outlined plan. It emphasizes the importance of patient awareness and collaboration. The Authorization for Treatment ensures patients are duly informed about the procedures and can make educated decisions regarding their healthcare, similar to the objectives of the Chiropractic Treatment Plan.
The Billing Information Form is also similar in its critical role within the healthcare interaction. This document gathers financial information and insurance details necessary for processing payments related to the treatments outlined in the Chiropractic Treatment Plan. While it does not directly address medical treatment, it is essential for facilitating the financial aspects of healthcare, ensuring patients are informed of their obligations and coverage.
Lastly, the Release of Information Form parallels the Chiropractic Treatment Plan by emphasizing patient consent regarding data sharing. This document allows healthcare providers to obtain and share necessary medical information between various parties, ensuring coordinated care. Like the Treatment Plan, it protects patient confidentiality while ensuring that relevant information is accessible for effective treatment planning and delivery.
When filling out the Chiropractic Treatment Plan form, following some simple dos and don’ts can make a significant difference in the quality and efficiency of your submission.
Misconceptions surrounding the Chiropractic Treatment Plan form can lead to misunderstandings among patients and practitioners alike. Here are four common misconceptions:
When filling out the Chiropractic Treatment Plan form, clarity and accuracy are paramount. Here are some key takeaways to keep in mind: