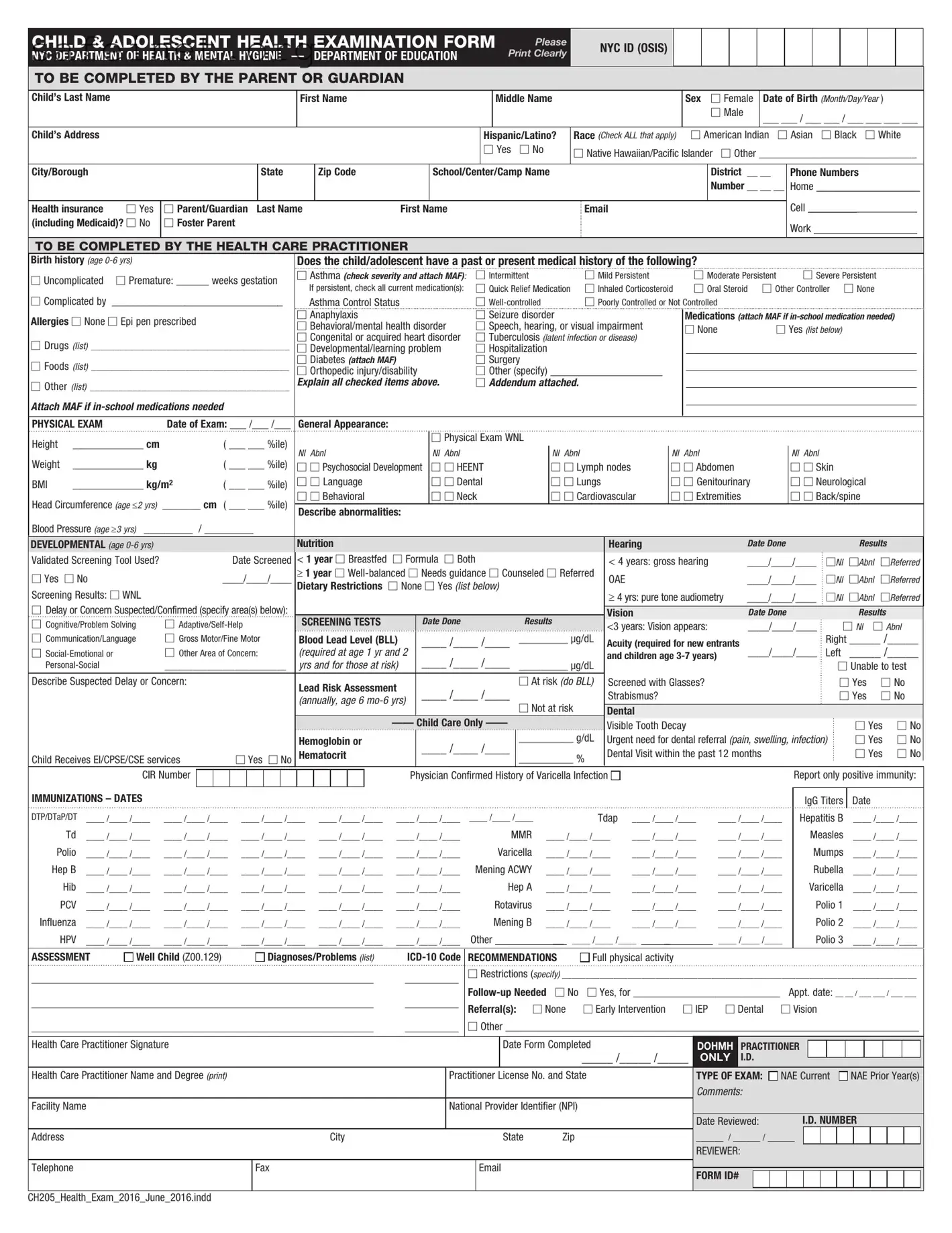
The Child Adolescent Health form is an essential resource for parents and guardians in New York City that helps ensure the health and well-being of children from infancy through adolescence. This comprehensive document gathers crucial information about a child's medical history, including vaccination records, birth history, and any existing health issues. Parents are prompted to provide details related to their child’s growth measurements, physical exam results, and developmental screenings. The form also addresses important health factors such as allergies, medication requirements, and specific developmental concerns. An important component is the section dedicated to the healthcare practitioner’s evaluation, which includes assessments of general appearance, nutrition, vision, and hearing capabilities. Collectively, this information empowers caregivers and educators to identify health needs and coordinate appropriate interventions, making the Child Adolescent Health form a pivotal tool in fostering a supportive environment for the growth of young individuals.
CHILD & ADOLESCENT HEALTH EXAMINATION FORM
NYC DEPARTMENT OF HEALTH & MENTAL HYGIENE — DEPARTMENT OF EDUCATION
Please Print Clearly
NYC ID (OSIS) 
TO BE COMPLETED BY THE PARENT OR GUARDIAN
Child’s Last Name
First Name
Middle Name
Sex ☐ Female
☐Male
Date of Birth (Month/Day/Year )
___ ___ / ___ ___ / ___ ___ ___ ___
Child’s Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hispanic/Latino? |
Race (Check ALL that apply) |
|
☐ American Indian ☐ Asian |
☐ Black |
☐ White |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐ Yes |
|
☐ No |
☐ Native Hawaiian/Pacific Islander |
☐ Other _____________________________ |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
City/Borough |
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|
|
School/Center/Camp Name |
|
|
|
|
|
|
|
|
|
District |
__ __ |
Phone Numbers |
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number __ __ __ |
Home ___________________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cell |
_________ |
|
|
|
|
|||||||||
Health insurance |
☐ Yes |
☐ Parent/Guardian Last Name |
|
|
|
|
|
First Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
(including Medicaid)? ☐ No |
☐ Foster Parent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE COMPLETED BY THE HEALTH CARE PRACTITIONER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
Birth history (age |
|
|
|
|
|
|
|
|
Does the child/adolescent have a past or present medical history of the following? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
☐ Uncomplicated ☐ Premature: ______ weeks gestation |
☐ Asthma (check severity and attach MAF): |
☐ Intermittent |
|
|
|
☐ Mild Persistent |
|
|
|
☐ Moderate Persistent |
|
☐ Severe Persistent |
|
|
|
||||||||||||||||||||||||||||||||||||||
|
If persistent, check all current medication(s): |
☐ Quick Relief Medication |
☐ Inhaled Corticosteroid |
|
☐ Oral Steroid ☐ Other Controller |
☐ None |
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
☐ Complicated by |
_________________________________ |
|
Asthma Control Status |
|
|
|
☐ |
|
|
|
☐ Poorly Controlled or Not Controlled |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
Allergies ☐ None ☐ Epi pen prescribed |
|
|
|
|
|
|
|
☐ Anaphylaxis |
|
|
|
|
☐ Seizure disorder |
|
|
|
|
|
|
|
Medications (attach MAF if |
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
☐ Behavioral/mental health disorder |
☐ Speech, hearing, or visual impairment |
|
|
☐ None |
|
☐ Yes (list below) |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
☐ Congenital or acquired heart disorder |
☐ Tuberculosis |
(latent infection or disease) |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
☐ Drugs (list) __________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
☐ Developmental/learning problem |
☐ Hospitalization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
☐ Foods (list) __________________________________________ |
☐ Diabetes (attach MAF) |
|
|
|
☐ Surgery |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
☐ Orthopedic injury/disability |
☐ Other (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
☐ Other (list) __________________________________________ |
Explain all checked items above. |
☐ Addendum attached. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
Attach MAF if |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
PHYSICAL EXAM |
|
Date of Exam: ___ /___ /___ |
General Appearance: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
Height |
_____________ cm |
|
|
( ___ ___ %ile) |
|
|
|
|
|
|
|
|
|
☐ Physical Exam WNL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
Nl |
Abnl |
|
|
|
Nl Abnl |
|
|
|
|
|
|
Nl Abnl |
|
|
|
|
|
Nl |
Abnl |
|
|
Nl Abnl |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
Weight |
_____________ kg |
|
|
( ___ ___ %ile) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
☐ ☐ Psychosocial Development |
☐ ☐ HEENT |
|
|
|
☐ ☐ Lymph nodes |
|
|
|
☐ ☐ Abdomen |
|
☐ ☐ Skin |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
BMI |
_____________ kg/m2 |
|
( ___ ___ %ile) |
☐ ☐ Language |
|
|
|
☐ ☐ Dental |
|
|
|
☐ ☐ Lungs |
|
|
|
☐ ☐ Genitourinary |
☐ ☐ Neurological |
|
|
|
|||||||||||||||||||||||||||||||||
Head Circumference (age ≤2 yrs) |
_______ cm ( ___ ___ %ile) |
☐ ☐ Behavioral |
|
|
|
☐ ☐ Neck |
|
|
|
☐ ☐ Cardiovascular |
|
☐ ☐ Extremities |
|
☐ ☐ Back/spine |
|
|
|
|
|||||||||||||||||||||||||||||||||||
Describe abnormalities: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Blood Pressure (age ≥3 yrs) _________ |
/ _________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
DEVELOPMENTAL (age |
|
|
|
|
|
|
|
|
Nutrition |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hearing |
|
|
|
|
|
|
|
Date Done |
|
|
|
|
|
|
Results |
|
|
||||||||||||
Validated Screening Tool Used? |
|
|
|
Date Screened |
< 1 year ☐ Breastfed |
☐ Formula ☐ Both |
|
|
|
|
|
|
|
< 4 years: gross hearing |
|
____/____/____ |
☐Nl |
|
☐Abnl |
☐Referred |
|||||||||||||||||||||||||||||||||
☐ Yes |
☐ No |
|
|
____/____/____ |
≥ 1 year ☐ |
|
OAE |
|
|
|
|
|
|
|
|
|
____/____/____ |
☐Nl |
|
☐Abnl |
☐Referred |
||||||||||||||||||||||||||||||||
Screening Results: ☐ WNL |
|
|
|
|
|
|
|
|
Dietary Restrictions |
☐ None ☐ Yes (list below) |
|
|
|
|
|
|
|
≥ 4 yrs: pure tone audiometry |
____/____/____ |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐Nl |
|
☐Abnl |
☐Referred |
||||||||||||||||||||||
☐ Delay or Concern Suspected/Confirmed (specify area(s) below): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vision |
|
|
|
|
|
|
|
Date Done |
|
|
|
|
|
|
Results |
|
|
||||||||||||||||
☐ Cognitive/Problem Solving |
☐ |
SCREENING TESTS |
|
|
Date Done |
|
|
|
|
Results |
|
|
<3 years: Vision appears: |
|
____/____/____ |
☐ Nl |
☐ Abnl |
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
☐ Communication/Language |
☐ Gross Motor/Fine Motor |
Blood Lead Level (BLL) |
|
____ /____ /____ |
|
_________ µg/dL |
|
Acuity (required for new entrants |
|
|
|
|
|
Right _____ /_____ |
|||||||||||||||||||||||||||||||||||||||
☐ |
☐ Other Area of Concern: |
(required at age 1 yr and 2 |
|
____ /____ /____ |
|
|
|
|
|
|
|
and children age |
|
____/____/____ |
Left |
_____ /_____ |
|||||||||||||||||||||||||||||||||||||
|
__________________________ |
yrs and for those at risk) |
|
|
_________ µg/dL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
☐ Unable to test |
|||||||||||||||||||||||||||||||
Describe Suspected Delay or Concern: |
|
|
|
|
|
|
|
Lead Risk Assessment |
|
____ /____ /____ |
|
☐ At risk (do BLL) |
Screened with Glasses? |
|
|
|
|
|
|
☐ Yes |
☐ No |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Strabismus? |
|
|
|
|
|
|
|
|
|
|
|
|
☐ Yes |
☐ No |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
(annually, age 6 |
|
|
☐ Not at risk |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dental |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
__________ g/dL |
|
Visible Tooth Decay |
|
|
|
|
|
|
|
|
☐ Yes |
☐ No |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Hemoglobin or |
|
|
____ /____ /____ |
|
|
Urgent need for dental referral (pain, swelling, infection) |
|
☐ Yes |
☐ No |
||||||||||||||||||||||||||||||||
Child Receives EI/CPSE/CSE services |
|
|
☐ Yes ☐ No |
Hematocrit |
|
|
|
__________ % |
|
Dental Visit within the past 12 months |
|
|
|
|
|
|
☐ Yes |
☐ No |
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
CIR Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Confirmed History of Varicella Infection |
|
|
|
|
|
|
|
|
|
|
|
Report only positive immunity: |
|||||||||||||||||||||||
IMMUNIZATIONS – DATES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IgG Titers |
|
Date |
|
|
|
||||||||
DTP/DTaP/DT |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
|
|
Tdap |
____ /____ /____ |
|
|
____ /____ /____ |
|
Hepatitis B |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
|
Td |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
|
MMR |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Measles |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||
Polio |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
Varicella |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Mumps |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||
Hep B |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
Mening ACWY |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Rubella |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||||
|
Hib |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
|
Hep A |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
Varicella |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
|
PCV |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
Rotavirus |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
|
Polio 1 |
____ /____ /____ |
|
||||||||||||||||||||||||||||||||||
Influenza |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
|
Mening B |
____ /____ /____ |
____ /____ /____ |
|
|
____ /____ /____ |
|
|
|
Polio 2 |
____ /____ /____ |
|
|||||||||||||||||||||||||||||||||||
|
HPV |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
____ /____ /____ |
Other |
|
|
|
__ |
|
____ /____ /____ |
|
_ |
|
|
|
|
____ /____ /____ |
|
|
|
Polio 3 |
____ /____ /____ |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
ASSESSMENT |
Well Child (Z00.129) |
|
|
|
Diagnoses/Problems (list) |
RECOMMENDATIONS |
Full physical activity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
☐Restrictions (specify) ____________________________________________________________________________
☐ Yes, for ___________________________ |
Appt. date: __ __ / ___ ___ / ___ ___ |
|||
Referral(s): ☐ None |
☐ Early Intervention |
☐ IEP |
☐ Dental |
☐ Vision |
☐Other ____________________________________________________________________________
Health Care Practitioner Signature |
|
|
|
Date Form Completed |
DOHMH |
|
PRACTITIONER |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
_____ /_____ /_____ |
ONLY |
|
I.D. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Health Care Practitioner Name and Degree (print) |
|
Practitioner License No. and State |
TYPE OF EXAM: |
|
NAE Current |
|
NAE Prior Year(s) |
||||||||||||||||||
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Facility Name |
|
National Provider Identifier (NPI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Date Reviewed: |
|
|
i.D. NUMBER |
||||||||||||||||
Address |
City |
|
|
State |
Zip |
______ / ______ / ______ |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
reviewer: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
Fax |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
FORM ID# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH205_Health_Exam_2016_June_2016.indd |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Fact Name | Description |
|---|---|
| Purpose of Form | The Child Adolescent Health Examination Form is used to gather health information about children and adolescents for school or camp enrollment in New York City. |
| Governing Body | This form is regulated by the New York City Department of Health and Mental Hygiene and the Department of Education. |
| Completion Requirement | It must be completed by a parent or guardian for students under 18 years old. |
| Medical History Section | The form includes a section for past or present medical conditions, including asthma, allergies, and developmental issues. |
| Physical Examination | A physical exam is required, during which height, weight, blood pressure, and other developmental assessments are documented. |
| Immunization Records | The form requests detailed immunization history, including vaccines administered and dates received for various illnesses. |
| Developmental Screening | It assesses various developmental domains such as communication, cognitive skills, and social-emotional growth. |
| Follow-Up Recommendations | Health care practitioners can provide recommendations for follow-up care based on their assessments and findings. |
| Signature Requirement | The form must be signed by a licensed health care practitioner as confirmation of examination and completion. |
Completing the Child Adolescent Health form is an important task that requires careful attention to detail. Each section of the form must be filled out accurately to ensure proper processing. Follow these steps to complete the form correctly and efficiently.
Once you have completed the form, review it carefully to ensure all information is accurate. This form is crucial for your child's health assessment and needs to be submitted promptly to prevent any delays in care or services. Please ensure all relevant sections are completed and nothing is missed.
What is the purpose of the Child Adolescent Health form?
The Child Adolescent Health form is designed to gather comprehensive health information about children and adolescents. It aids health care practitioners in assessing a child's health status, identifying potential issues, and ensuring that appropriate support services are available. The form is useful for schools, camps, and other settings where child welfare is a priority.
Who needs to complete the Child Adolescent Health form?
The form should be completed by a parent or guardian of the child. This includes natural parents, step-parents, or legal guardians. Foster parents can also fill it out. Accurate and complete information is essential for proper assessment and care.
What information is required from parents or guardians?
Parents or guardians need to provide essential details like their child's name, date of birth, address, school, and contact information. They will also indicate the child's health insurance status, ethnicity, and any notable medical history. This foundation helps health care providers offer tailored care.
What medical history details are requested on the form?
The form asks about significant medical history, such as past conditions like asthma, diabetes, allergies, and psychiatric issues. It also requires information about any past surgeries, hospitalizations, and developmental or learning issues. Providing this information enables better health management and intervention when necessary.
How is the physical exam section structured?
The physical exam section allows health care practitioners to assess various aspects of a child's health, including general appearance, height and weight percentiles, and specific system checks (like lungs and cardiovascular health). This part helps to establish a baseline and identify any abnormalities.
What developmental screenings are included in the form?
Developmental screenings assess different areas of a child's growth, including nutrition, hearing, vision, and cognitive development. The form also checks for any immediate concerns or indicators that could lead to further evaluation. These screenings help ensure that children are developing at a healthy pace.
What immunization records need to be provided?
The form requires detailed immunization history, listing dates for various vaccinations like DTP, MMR, and Polio. This information is crucial to ensure that children receive all necessary immunizations for their age, helping to prevent the spread of infectious diseases in schools and communities.
What happens after the form is completed?
Once the form is filled out, it should be submitted to the designated health care practitioner or school authority. They will review the information, conduct a health examination, and may recommend further follow-up or referrals if needed. This process supports ongoing monitoring of the child's health.
Can the form be updated if the child's health status changes?
Yes, the form can and should be updated if there are significant changes in the child's health, such as new diagnoses, changes in medications, or new allergies. Keeping this information current is vital for ongoing health management and transparency with healthcare providers.
Where can parents or guardians obtain the Child Adolescent Health form?
The Child Adolescent Health form is usually available through schools, health care providers, and the NYC Department of Health and Mental Hygiene. You can also download the form from official health department websites. Be sure to use the latest version for the most accurate and relevant information.
Inconsistent Information: Ensure that all details, such as the child's name and date of birth, are consistent across forms. Incorrect or differing information may lead to confusion or processing delays.
Incomplete Sections: Fill out every applicable section completely. Missing information can hinder the evaluation of the child’s health and may require additional follow-up.
Neglecting Required Attachments: It's essential to attach any necessary Medical Authorization Forms (MAF) when in-school medications are indicated. Omitting these can delay necessary medical care.
Using Inaccurate Medical Histories: Providing inaccurate or outdated information regarding the child’s past medical history may result in inappropriate recommendations or treatment plans. Always verify details before submission.
Failure to Indicate Allergies: If the child has any allergies, especially to medications, they must be clearly indicated on the form. This information is crucial to avoid potential health risks.
Improper Signature: Ensure that the appropriate guardian or parent signs the form. A missing or incorrect signature can render the form invalid, causing disruptions in care.
When addressing a child's health needs, there are several important forms and documents that complement the Child Adolescent Health form. Each of these documents plays a vital role in gathering relevant information about a child's overall well-being. Below is a list of such forms, along with a brief description of their purpose.
These forms collectively contribute to a holistic understanding of a child's health needs. They ensure that health care providers have the information necessary to deliver safe and effective care. Taking the time to complete these documents is a crucial step in supporting a child’s health journey.
The Child and Adolescent Health Examination Form shares similarities with the School Health Form, often required by educational institutions. Both documents gather essential information regarding a child’s health history, demographic information, and any existing medical conditions. Parents or guardians complete similar sections regarding the child's name, birth date, and pertinent medical history, ensuring a comprehensive understanding of each child's health needs as they enter or participate in school programs.
Another comparable document is the Well Child Visit form. This form focuses specifically on routine health checkups for children. Like the Child and Adolescent Health Examination Form, it includes sections for vaccination records, developmental milestones, and any ongoing health issues. The goal is to track the child's growth and health status over time, providing a similar overview of health conditions and necessary follow-ups.
The Immunization Record is also akin to the Child and Adolescent Health Examination Form. Both collect information on a child's vaccination history, ensuring that essential immunizations are up to date. This document plays a vital role in protecting public health, much like the examination form, which assures that children are monitored for their immunization status during health assessments.
The Behavioral Health Assessment form mirrors the Child and Adolescent Health Examination Form in that both documents address mental and emotional wellbeing. Each form typically includes screening questions for behavioral health issues and information regarding any past or present mental health conditions. This allows healthcare providers to assess and address both physical and mental health aspects in children.
The Consent for Treatment form can also be viewed as similar. Parents or guardians complete this document, granting permission for their child to receive medical attention. This is important for both addressing immediate health concerns and ensuring that any ongoing treatments align with the health information gathered in the Child and Adolescent Health Examination Form, fostering a cohesive approach to care.
Additionally, the Physical Examination Report is another document with similarities. It provides an overview of the child's physical health, much like the examination form. It includes vital signs, growth measurements, and results from various screenings. Both forms serve to create comprehensive medical records, facilitating informed decision-making for future healthcare needs.
The Special Education Eligibility form aligns closely, especially when detailing developmental or learning delays. It requires information about the child's overall health and developmental status, similar to the comprehensive evaluations found in the Child and Adolescent Health Examination Form. Both documents play a role in determining the services a child may need to thrive in an educational setting.
Lastly, the Annual Health Assessment form for camps and recreational programs addresses similar aspects. It collects data related to a child's medical history, immunizations, and health screenings, aiming to ensure safety and preparedness in group settings. Much like the Child and Adolescent Health Examination Form, it ensures that children participating in these activities are healthy and fit for their environments.
Do's:
Don'ts:
This form is essential for all children and adolescents, regardless of their current health status. It provides a comprehensive overview that helps healthcare providers ensure well-rounded care.
While it is often required for school enrollment, the form is also used for camps, sports, and other activities. It ensures that all caregivers are aware of the child's health needs.
Parents are encouraged to consult with healthcare providers when completing the form. This collaborative approach ensures accuracy and completeness in the child's health history.
Despite its length, every section plays a crucial role in assessing a child's health and development. The information helps create tailored health plans and interventions.
While the form is vital for establishing health records, it does not automatically guarantee immediate access to healthcare services. Other factors may still influence appointment availability and care access.
The Child Adolescent Health form plays a crucial role in gathering important health information for children and adolescents. Here are key takeaways for effectively completing and utilizing the form:
Following these guidelines enhances the utility of the Child Adolescent Health form, which in turn supports the health and well-being of the child.