The CHAMPVA Claim Form VA 10-7959A is a crucial document for veterans and their families seeking medical benefits under the Civilian Health and Medical Program of the Department of Veterans Affairs (CHAMPVA). Designed specifically for use by patients, sponsors, or guardians, this claim form must be completed in full to initiate the claims process. One important aspect to consider is that it is mandatory for all beneficiary claims, and it should not be used for claims submitted directly by healthcare providers. Timely filing is emphasized; claims must reach the CHAMPVA office no later than one year after the date of service or, for inpatient care, within one year of discharge. The form also requires beneficiaries to provide information about any other health insurance coverage they may have, as CHAMPVA typically acts as a secondary payer. Essential documentation must accompany the form, including itemized billing statements that detail services rendered, charges incurred, and appropriate medical coding. This article will delve deeper into how to accurately complete the form, the necessary supporting documents, and tips to ensure a smooth claims process.
|
|
OMB Number: |
|
|
|
|
|
CHAMPVA Claim Form |
VA Health Administration Center |
CHAMPVA PO Box 469064 Denver CO |
|
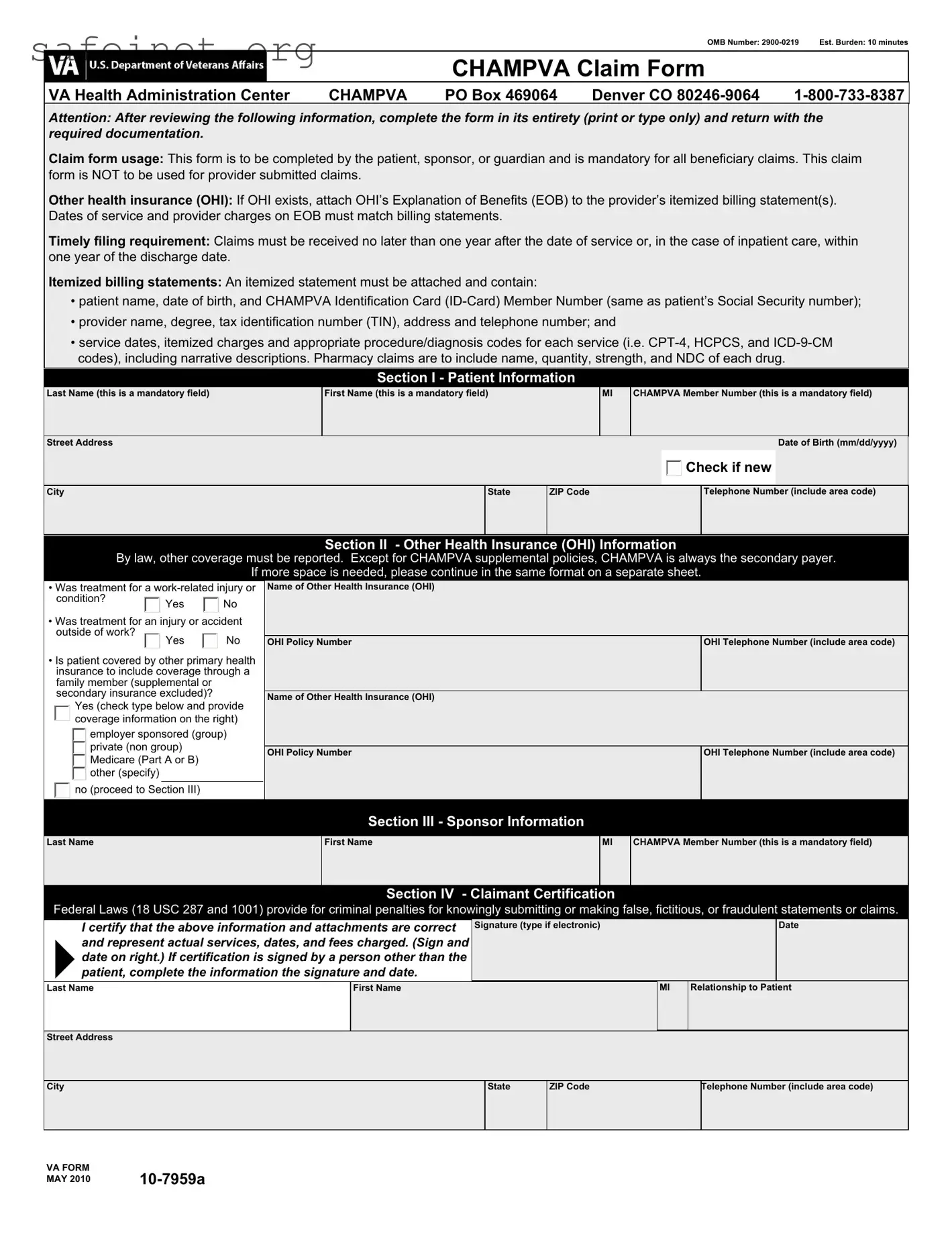
Attention: After reviewing the following information, complete the form in its entirety (print or type only) and return with the required documentation.
Claim form usage: This form is to be completed by the patient, sponsor, or guardian and is mandatory for all beneficiary claims. This claim form is NOT to be used for provider submitted claims.
Other health insurance (OHI): If OHI exists, attach OHI’s Explanation of Benefits (EOB) to the provider’s itemized billing statement(s). Dates of service and provider charges on EOB must match billing statements.
Timely filing requirement: Claims must be received no later than one year after the date of service or, in the case of inpatient care, within one year of the discharge date.
Itemized billing statements: An itemized statement must be attached and contain:
•patient name, date of birth, and CHAMPVA Identification Card
•provider name, degree, tax identification number (TIN), address and telephone number; and
•service dates, itemized charges and appropriate procedure/diagnosis codes for each service (i.e.
Section I - Patient Information
Last Name (this is a mandatory field)
First Name (this is a mandatory field)
MI
CHAMPVA Member Number (this is a mandatory field)
Street Address |
|
Date of Birth (mm/dd/yyyy) |
 Check if new
Check if new
City
State
ZIP Code
Telephone Number (include area code)
Section II - Other Health Insurance (OHI) Information
By law, other coverage must be reported. Except for CHAMPVA supplemental policies, CHAMPVA is always the secondary payer.
If more space is needed, please continue in the same format on a separate sheet.
• Was treatment for a
condition? |
Yes |
No |
|
•Was treatment for an injury or accident outside of work?
Yes |
No |
•Is patient covered by other primary health insurance to include coverage through a family member (supplemental or secondary insurance excluded)?
Yes (check type below and provide coverage information on the right)
 employer sponsored (group) private (non group)
employer sponsored (group) private (non group)
 Medicare (Part A or B) other (specify)
Medicare (Part A or B) other (specify)

 no (proceed to Section III)
no (proceed to Section III)
Name of Other Health Insurance (OHI)
|
|
OHI Policy Number |
OHI Telephone Number (include area code) |
|
|
|
|
Name of Other Health Insurance (OHI)
OHI Policy Number |
OHI Telephone Number (include area code) |
|
|
Section III - Sponsor Information
Last Name
First Name
MI
CHAMPVA Member Number (this is a mandatory field)
Section IV - Claimant Certification
Federal Laws (18 USC 287 and 1001) provide for criminal penalties for knowingly submitting or making false, fictitious, or fraudulent statements or claims.
I certify that the above information and attachments are correct and represent actual services, dates, and fees charged. (Sign and
4date on right.) If certification is signed by a person other than the
patient, complete the information the signature and date.
Signature (type if electronic)
Date
Last Name
First Name
|
MI |
Relationship to Patient |
|
|
|
Street Address
City
State
ZIP Code
Telephone Number (include area code)
VA FORM |
|
MAY 2010 |
CHAMPVA Claim Form
Notice: Termination of marriage by divorce or annulment to the qualifying sponsor ends CHAMPVA eligibility as of midnight on the effective date of the dissolution of marriage. Changes in status should be reported immediately to CHAMPVA, ATTN: Eligibility Unit, PO Box 469028, Denver, CO
PRIVACY ACT INFORMATION: The authority for collection of the requested information on this form is 38 U.S.C. 501 and 1781. The purpose of collecting this information is to adjudicate and process claims for CHAMPVA benefits. You do not have to provide the requested information but if any or all of the requested information is not provided, it may delay or result in denial of your request for CHAMPVA benefits. Failure to furnish the requested information will have no adverse impact on any other VA benefit to which you may be entitled. The responses you submit are considered confidential and may be disclosed outside VA only if the disclosure is authorized under the Privacy Act, including the routine uses identified in the VA system of records 54VA16, titled "Health Administration Center Civilian Health and Medical Program Records
PAPERWORK REDUCTION ACT: This information collection is in accordance with the clearance requirements of Section 3507 of the Paperwork Reduction Act of 1995. Public reporting burden for this collection of information is estimated to average 10 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed and completing and reviewing the collection of information. Comments regarding this burden estimate or any other aspect of this collection, including suggestions for reducing the burden, may be addressed by calling the CHAMPVA Help Line,
VA FORM |
|
MAY 2010 |
| Fact | Description |
|---|---|
| Form Identification | The CHAMPVA Claim Form is officially known as VA Form 10-7959A and is designated for beneficiaries seeking to claim CHAMPVA benefits. |
| Required Documentation | Beneficiaries must complete the form in its entirety and attach necessary documents, including itemized billing statements and any applicable Explanation of Benefits from other health insurance. |
| Timely Filing | Claims should be submitted no later than one year from the date of service, or within one year of discharge for inpatient care. |
| Patient Information | Section I requires patient-specific details like name, date of birth, and CHAMPVA member number. All fields indicated as mandatory must be completed. |
| Legal Authority | The collection of information on this form is authorized under 38 U.S.C. 501 and 1781, which enables the processing of claims for CHAMPVA benefits. |
After gathering the necessary documentation for your claim, it is important to complete the CHAMPVA Claim Form (VA 10-7959A) accurately. Following the steps below will ensure you provide the required information for processing.
Double-check all information for accuracy to avoid any delays in processing your claim. Claims must be submitted within one year of service or discharge to ensure timely review. If you have questions while completing the form, don't hesitate to reach out for assistance.
What is the purpose of the CHAMPVA Claim VA 10-7959A form?
The CHAMPVA Claim VA 10-7959A form is used to submit claims for benefits under the CHAMPVA program. This form should be completed by the patient, their sponsor, or their guardian. It's important to note that this form is mandatory for all beneficiary claims and not intended for claims submitted by healthcare providers.
Who should complete the form?
The form should be completed by the patient, the sponsor (typically a veteran), or a legal guardian of the patient. It is crucial that all required information is printed or typed clearly. This ensures that the claim can be processed smoothly and without delay.
What information needs to be included on the form?
What are the timely filing requirements for submitting claims?
To be eligible for benefits, claims must be submitted within one year of the date services were provided. If the claim involves inpatient care, it must be submitted within one year of the patient’s discharge date. Failure to adhere to these deadlines can result in denial of the claim.
What should I do if the patient has other health insurance?
If the patient has other health insurance (OHI), it is mandatory to report it on the form. Attach the OHI's Explanation of Benefits (EOB) to the claim, ensuring that the service dates and charges match the itemized billing statements from the provider. CHAMPVA acts as a secondary payer, so all coordination of benefits must be clearly indicated.
What documentation must be submitted with the claim form?
When submitting the form, you must include an itemized billing statement. This statement should contain the patient's name, date of birth, CHAMPVA Member Number, the provider's details, service dates, itemized charges, and all relevant procedure and diagnosis codes. Pharmacy claims should list the name, quantity, strength, and National Drug Code (NDC) for each medication.
What steps should be taken if marital status changes?
If the sponsor’s marital status changes due to divorce or annulment, CHAMPVA eligibility ceases at midnight on the date of the dissolution. It is important to report such changes immediately to CHAMPVA to avoid any issues with claims or coverage.
What are the privacy considerations with this form?
Your submitted information is considered confidential. It may be shared outside of the VA only if authorized under the Privacy Act. The information provided can help determine eligibility for benefits, but all disclosures will comply with privacy regulations to protect your personal data.
How long does it take to complete the CHAMPVA Claim VA 10-7959A form?
On average, completing the form should take about 10 minutes. This estimate includes the time needed to review the instructions, gather necessary documents, and fill out the form accurately. It is advisable to prepare all information ahead of time to streamline the process.
Incomplete Personal Information: Failing to fill in all mandatory fields, such as the patient's last name, first name, and CHAMPVA Member Number.
Missing Dates: Not including the date of birth in the correct format (mm/dd/yyyy) can lead to processing delays.
Incorrect Reporting of Other Health Insurance: Not disclosing any existing Other Health Insurance (OHI) can result in claims being denied.
Improper Documentation: Failing to attach the required itemized billing statements and missing details such as service dates or procedure codes may delay processing.
Invalid Submission for Provider Claims: Using the form for provider-submitted claims instead of patient claims is a common error.
Ignoring Timely Filing Requirements: Submitting claims after one year from the date of service or discharge can lead to automatic denial.
Failure to Certify: Not providing a signature or date in the certification section can leave the claim incomplete and unprocessed.
The CHAMPVA Claim Form VA 10-7959A is a fundamental document for claiming benefits. To effectively submit claims, several other forms and documents may be required. Below is a list of these essential documents, each with a brief description.
Submitting a CHAMPVA claim requires careful attention to detail and the inclusion of all necessary documents. Ensuring that all paperwork is complete and accurate can help expedite the claims process.
The CHAMPVA Claim Form VA 10-7959A is similar to the Medicare Claim Form, also known as the CMS-1500. Both forms serve the critical function of processing claims for medical benefits in a clear, standardized way. Like the CHAMPVA form, the Medicare Claim Form requires detailed patient information including the patient's name, identification number, and relevant health insurance details. The structure encourages accuracy, as it must be completed thoroughly to ensure prompt processing of the claim.
Another document that parallels the CHAMPVA Claim Form is the Blue Cross Blue Shield Claim Form. Similar to the previous forms, it is intended for members to submit claims for reimbursement of medical expenses. Both forms are designed to collect essential details such as date of service, provider information, and itemized charges. In this manner, they help streamline the claims process between health insurance companies and healthcare providers.
The TRICARE Claim Form is also quite comparable to the CHAMPVA Claim Form. TRICARE covers service members and their families, and their claim form serves a similar purpose: to allow beneficiaries to seek reimbursement for covered medical expenses. They require similar pieces of information, such as patient identification, service dates, and charges, ensuring consistency across the different forms. This uniformity helps ease the burden on patients and healthcare providers alike.
Another important document is the Health Insurance Claim Form (also known as the UB-04). This form is particularly used by hospitals and institutional providers to submit claims for payments. Like the CHAMPVA Claim Form, it gathers comprehensive details such as patient information, treatment codes, and provider details. While the UB-04 is typically used for institutional claims rather than individual claims, the similarities in information requirements highlight the need for clarity in claims processing.
The Workers' Compensation Claim Form is yet another example that shares features with the CHAMPVA Claim Form. This form is specifically designed for individuals who have been injured at work and need to file for benefits. It includes sections for patient information, a brief summary of the injury or accident, and medical treatment received. This overlap in structure emphasizes the importance of collecting accurate and complete information to facilitate the claims process, similar to how CHAMPVA operates.
The VA Form 21-526EZ is used for veterans to apply for disability compensation but shares elements with the CHAMPVA Claim Form. It requires personal details and information on prior medical history, affirming the need for comprehensive data in both applications. Although the purposes differ—one is for initiating claims and the other for reimbursement—the organization of required information remains similar.
Finally, the Flexible Spending Account (FSA) Claim Form is akin to the CHAMPVA Claim Form in that it allows individuals to seek reimbursement for qualified medical expenses. Just like the CHAMPVA form, it requires documentation like itemized statements and proof of service dates. Both forms necessitate thorough completion to ensure that claims are processed efficiently, making them vital to managing healthcare costs.
Things to Do:
Things Not to Do:
Misconceptions surrounding the CHAMPVA Claim VA 10-7959A form can often lead to confusion for beneficiaries. Understanding the truth behind these misconceptions is important for a smoother claims process. Here are ten common misconceptions clarified:
Addressing these misconceptions can help beneficiaries navigate the claims process more effectively and ensure timely access to the benefits they are entitled to under CHAMPVA.