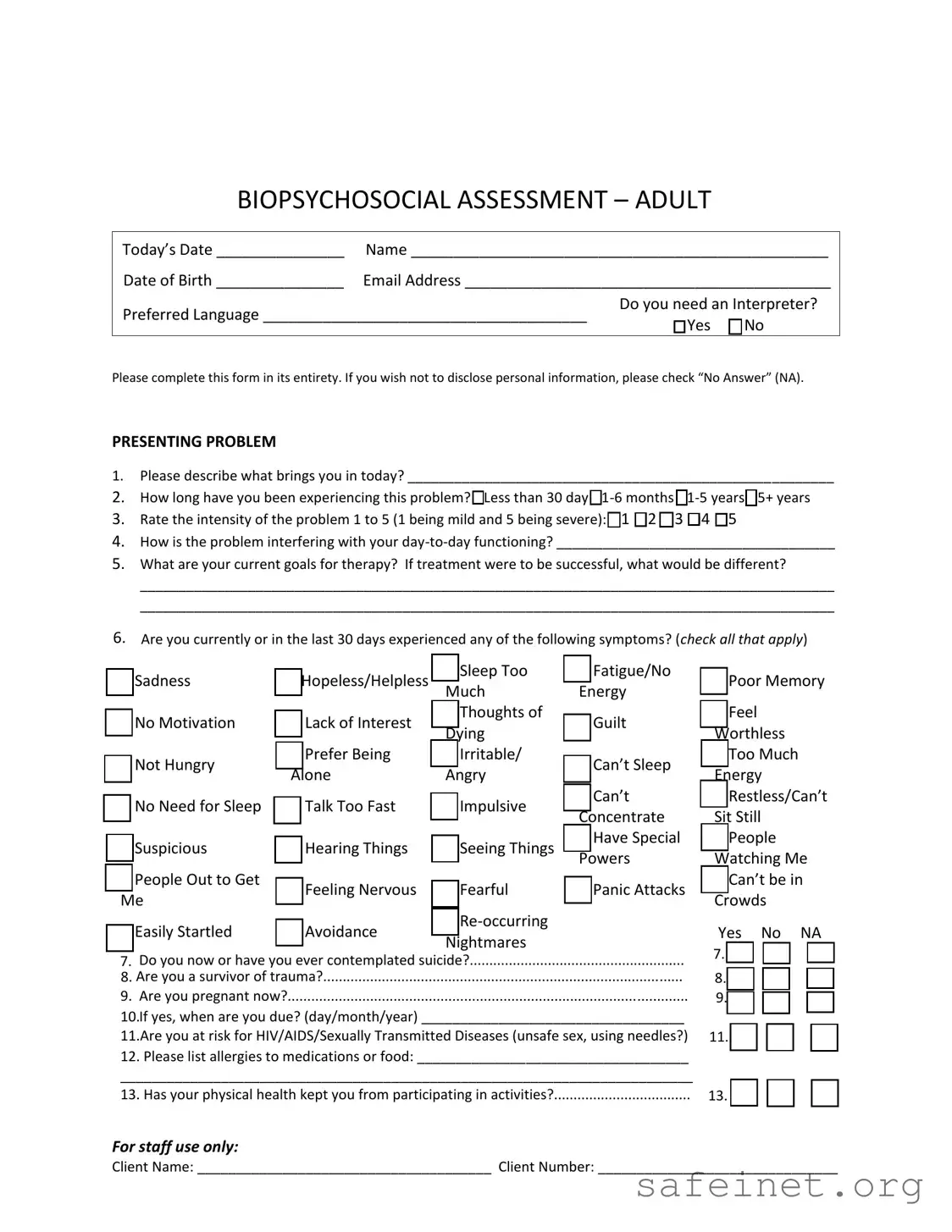
The Biopsychosocial Assessment Social Work form serves as a comprehensive tool designed to gather crucial information about an individual's mental, physical, and social well-being. This form begins with basic demographic details, including the person's name, date of birth, and preferred language, ensuring that communication barriers are addressed, especially for those needing an interpreter. The assessment delves into the presenting problem, prompting individuals to articulate their concerns and the duration of these issues. It encourages clients to rate the intensity of their problems and to reflect on how these challenges impact their daily lives and therapy goals. Furthermore, it explores symptoms experienced in the past month, any history of suicidal thoughts or trauma, and current health risks, including HIV/AIDS. Substance use and addiction are also assessed, both currently and historically, alongside family dynamics and relationships. The form addresses education and legal history, providing a holistic view of the individual's life circumstances. Lastly, it examines work history and medical background, including past interactions with mental health professionals. This thorough approach not only aids social workers in understanding the client’s situation but also facilitates a more tailored therapeutic process.
| Fact Name | Description |
|---|---|
| Purpose | The Biopsychosocial Assessment is designed to gather comprehensive information about an individual's mental health, social environment, and physical health. |
| Client Information | It requires personal details, such as name, date of birth, and preferred language, to ensure effective communication and understanding. |
| Presenting Problem | The form prompts clients to describe their current issues, including duration and impact on daily life, allowing for targeted treatment planning. |
| Symptoms Checklist | A checklist of symptoms helps identify mental health concerns, such as sadness, anxiety, or suicidal thoughts, ensuring thorough assessment. |
| Legal Considerations | In states like California, the assessment adheres to the California Business and Professions Code, ensuring compliance with mental health regulations. |
| Family and Relationships | The assessment explores family dynamics and support systems, which are crucial for understanding the client's social context and potential influences on their well-being. |
Completing the Biopsychosocial Assessment Social Work form is an essential step in providing the necessary information for effective support. The following steps will guide you through filling out the form accurately and thoroughly.
What is a Biopsychosocial Assessment?
A Biopsychosocial Assessment is a comprehensive evaluation used in social work to understand an individual's biological, psychological, and social factors that may affect their well-being. This assessment helps professionals identify the root causes of issues and develop a tailored treatment plan. It covers various aspects of a person's life, including health, relationships, and personal history.
Why is it important to complete the assessment thoroughly?
Completing the assessment thoroughly is crucial for several reasons. First, it provides a complete picture of your situation, which can lead to more effective treatment. Second, it helps the social worker understand your needs and preferences better. Lastly, being open and honest can foster a stronger therapeutic relationship, ultimately benefiting your overall progress in therapy.
What should I do if I don't want to disclose certain information?
If you're uncomfortable sharing specific details, you can select "No Answer" (NA) for those questions. It's essential to remember that your comfort and safety are priorities. The assessment is designed to help you, and you should only share what you feel ready to discuss.
How does the assessment address mental health concerns?
The assessment includes questions about your mental health history, current symptoms, and any past experiences with mental health professionals. By identifying these factors, the social worker can better understand your mental health needs and develop an appropriate treatment plan. It also helps identify any urgent concerns that may need immediate attention.
What happens after I complete the assessment?
Once you complete the assessment, the social worker will review your responses and discuss them with you. Together, you will identify goals for therapy and create a plan tailored to your needs. This collaborative approach ensures that you are actively involved in your treatment and that it aligns with your personal goals.
Failing to complete the form in its entirety. Each section is important for understanding your situation.
Not providing specific details about your presenting problem. General statements can lead to misunderstandings.
Neglecting to indicate the duration of the problem. This information helps professionals gauge the severity and urgency.
Skipping the intensity rating. This helps in assessing how much the problem affects your daily life.
Overlooking symptoms that may seem minor. Even small issues can contribute to a larger picture.
Not disclosing past or current suicidal thoughts. This is crucial for your safety and well-being.
Forgetting to list any allergies to medications or food. This can prevent adverse reactions during treatment.
Failing to mention any significant life changes. Recent events can have a major impact on mental health.
Not being honest about substance use or addiction history. Transparency is key for effective treatment.
Ignoring the importance of relationships. Family dynamics can significantly affect mental health.
The Biopsychosocial Assessment Social Work form is a critical document used in social work practice to gather comprehensive information about an individual's psychological, social, and biological factors. Several other forms and documents often accompany this assessment to provide a holistic view of the client's situation. Below is a list of these forms, each described briefly for clarity.
These documents work together to create a comprehensive understanding of the client’s needs and circumstances. Properly utilizing these forms enhances the effectiveness of the social work process and supports the client's journey toward well-being.
The Biopsychosocial Assessment Social Work form shares similarities with the Mental Health Intake Form. Both documents aim to gather comprehensive information about an individual's mental health status and personal history. They typically include sections on presenting problems, symptoms, and any relevant medical history. The Mental Health Intake Form often focuses more on the psychological aspects, while the Biopsychosocial Assessment includes social and biological factors as well.
Another document that resembles the Biopsychosocial Assessment is the Substance Abuse Assessment. This form specifically addresses issues related to alcohol and drug use, including patterns of use and consequences. Like the Biopsychosocial Assessment, it explores the impact of substance use on an individual’s life, including relationships and daily functioning. Both assessments aim to identify underlying issues that may contribute to a person’s struggles.
The Family Assessment form also shares common ground with the Biopsychosocial Assessment. It focuses on family dynamics, relationships, and support systems. This document often includes questions about family history, conflicts, and significant life changes. By understanding family interactions, social workers can better assess how these factors influence an individual’s mental health and overall well-being.
The Psychological Evaluation form is similar in its goal of understanding a client’s mental health. It typically includes standardized tests and assessments to evaluate cognitive and emotional functioning. While the Biopsychosocial Assessment collects qualitative data through open-ended questions, the Psychological Evaluation often relies on quantitative measures to provide a more structured analysis of mental health issues.
The Health History Questionnaire is another document that aligns with the Biopsychosocial Assessment. It gathers information about a person’s medical history, current health status, and medications. Both forms aim to understand how physical health impacts mental well-being. The Health History Questionnaire may not delve as deeply into social factors, but it is crucial for a holistic understanding of a client’s situation.
The Client Risk Assessment form is akin to the Biopsychosocial Assessment in that it evaluates potential risks a client may face. This document often includes questions about suicidal thoughts, self-harm, and other safety concerns. Both assessments aim to identify critical areas that require immediate attention, ensuring the safety and well-being of the client.
The Social History Form is another document that shares similarities. It collects information about a person’s background, including upbringing, education, and life experiences. Like the Biopsychosocial Assessment, it seeks to understand how these factors contribute to current challenges. Both forms emphasize the importance of context in assessing an individual’s mental health.
Lastly, the Treatment Plan is closely related to the Biopsychosocial Assessment. While the latter gathers information to inform treatment, the Treatment Plan outlines specific goals and interventions based on the assessment findings. Both documents are essential in the therapeutic process, ensuring that the client’s needs are addressed in a comprehensive manner.
When filling out the Biopsychosocial Assessment Social Work form, consider the following do's and don'ts:
Here are five common misconceptions about the Biopsychosocial Assessment Social Work form:
Completing the Biopsychosocial Assessment is essential for understanding an individual’s unique situation. It covers various aspects of life, including emotional, social, and physical health.
Be thorough when describing the presenting problem. This section sets the stage for therapy and helps identify the main issues that need to be addressed.
It’s important to rate the intensity of the problem accurately. This helps the therapist gauge the severity and prioritize treatment accordingly.
Honesty is crucial when answering questions about substance use and mental health symptoms. This information is vital for creating an effective treatment plan.
Consider the relationships section carefully. Understanding family dynamics and support systems can provide valuable insights into personal challenges and strengths.