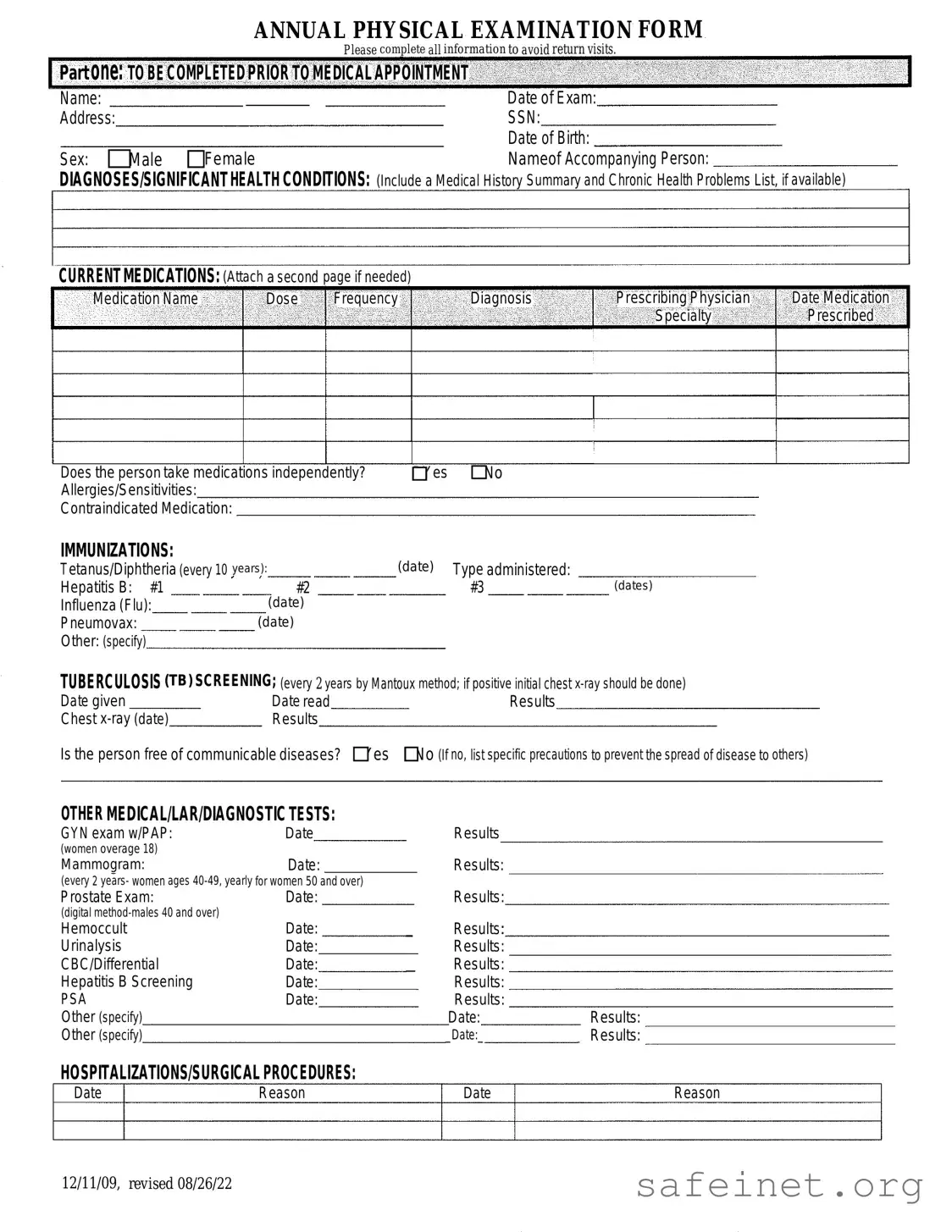
The Annual Physical Examination form serves as a crucial tool in promoting patient health and ensuring that medical professionals have the necessary information to provide effective care. This form is divided into two main parts, each designed to gather specific details about the patient’s medical history and current health status. In the first part, patients must complete essential personal information, including their name, date of birth, and address, as well as details about any significant health conditions and current medications. This section also requires information about allergies, immunizations, and recent medical tests. The second part focuses on the general physical examination, where vital signs such as blood pressure, pulse, and temperature are recorded. Additionally, a systematic evaluation of various body systems is conducted, allowing healthcare providers to identify any abnormalities. The form also includes space for comments on further evaluations, recommendations for health maintenance, and any limitations on activities. By completing this form accurately, patients can help ensure a comprehensive assessment during their annual physical examination, ultimately fostering a proactive approach to their health and well-being.
| Fact Name | Description |
|---|---|
| Purpose | The Annual Physical Examination form is designed to collect comprehensive health information from patients prior to their medical appointments. |
| Patient Information | Patients must provide personal details, including name, date of birth, address, and Social Security Number, to ensure accurate medical records. |
| Health History | The form requires a summary of significant health conditions and current medications, which assists healthcare providers in making informed decisions. |
| Immunization Records | Patients must document their immunization history, including dates for Tetanus, Hepatitis B, and Influenza vaccinations, among others. |
| TB Screening | TB screening is mandated every two years using the Mantoux method, with specific instructions for follow-up if results are positive. |
| State-Specific Laws | In some states, such as California, the governing law requires that certain medical history disclosures be made available to healthcare providers under the Health and Safety Code. |
| Physical Examination | The form includes a section for vital signs and a general physical examination, which helps in evaluating the patient's overall health status. |
| Special Instructions | Recommendations for health maintenance, dietary needs, and limitations or restrictions for activities must be documented to guide patient care. |
| Signature Requirement | A physician's signature is required at the end of the form to validate the examination and the information provided by the patient. |
Completing the Annual Physical Examination form is a straightforward process. This form gathers essential information about your health history, current medications, and any significant medical conditions. By filling it out accurately, you help ensure that your healthcare provider has the necessary details to offer you the best care possible.
What is the purpose of the Annual Physical Examination form?
The Annual Physical Examination form is designed to collect comprehensive health information from individuals prior to their medical appointments. This information helps healthcare providers evaluate a patient's health status, medical history, and current medications, ensuring that appropriate care is provided during the visit.
Who needs to complete the form?
All individuals seeking a physical examination should complete the form. This includes new patients as well as those returning for annual check-ups. Completing the form accurately helps to avoid delays or return visits due to missing information.
What information is required in Part One of the form?
Part One requires personal details such as name, date of exam, address, social security number, date of birth, and sex. Additionally, individuals must provide information about any significant health conditions, current medications, allergies, immunizations, and any recent medical tests. This section is critical for establishing a comprehensive health profile.
What should be included in the section about current medications?
In the current medications section, individuals should list all medications they are taking, including the name, dosage, frequency, diagnosis for which the medication was prescribed, and the prescribing physician's name. If necessary, a second page may be attached for additional medications. Indicating whether the person takes medications independently is also important.
How often should tuberculosis (TB) screening be conducted?
TB screening should be conducted every two years using the Mantoux method. If the initial screening result is positive, a chest x-ray should be performed to further evaluate the individual's health status.
What types of immunizations should be documented?
The form requires documentation of several immunizations, including Tetanus/Diphtheria (every 10 years), Hepatitis B (three doses), Influenza (annual), and Pneumovax (as recommended). Any additional immunizations should also be specified in the form.
What information is gathered in the General Physical Examination section?
The General Physical Examination section collects vital signs, including blood pressure, pulse, respirations, temperature, height, and weight. It also evaluates various body systems, noting whether normal findings were observed and if further evaluation is recommended by a specialist.
What should individuals do if there has been a change in their health status from the previous year?
If there has been a change in health status, individuals should specify the details in the designated section of the form. This information is crucial for healthcare providers to understand any new health concerns and adjust care plans accordingly.
How can individuals ensure their information is kept confidential?
Individuals should ensure that the form is completed in a private setting and submitted directly to their healthcare provider. Providers are required to adhere to privacy laws, such as HIPAA, which protect personal health information from unauthorized access.
Incomplete Personal Information: Failing to fill in all required fields such as name, date of birth, and address can lead to delays in processing the form.
Missing Medical History: Not providing a summary of significant health conditions or chronic problems may result in inadequate care during the examination.
Inaccurate Medication Details: Omitting current medications or incorrectly listing dosages can lead to serious health risks. Always double-check this section.
Neglecting Allergies: Failing to disclose allergies or sensitivities can jeopardize patient safety. This information is crucial for avoiding adverse reactions.
Ignoring Immunization Records: Not including dates of immunizations or failing to note if they are up to date can affect the patient's eligibility for certain treatments.
Overlooking Screening Tests: Not documenting results of required screenings, such as TB tests or mammograms, can lead to missed health issues.
Failure to Update Health Changes: Not indicating any changes in health status from the previous year may prevent the physician from providing the best care possible.
When preparing for an annual physical examination, several other forms and documents may be needed. These documents help provide a comprehensive view of a patient's health and medical history. Here is a list of commonly used forms alongside the Annual Physical Examination form.
These forms and documents work together to provide healthcare providers with a clear picture of a patient's health status. Having them prepared in advance can lead to a more efficient and effective medical appointment.
The Annual Health Questionnaire is similar to the Annual Physical Examination form in that both documents collect comprehensive health information from patients. The Annual Health Questionnaire typically includes sections for personal details, medical history, current medications, and any known allergies. This document serves as a preliminary assessment tool, allowing healthcare providers to gather essential data before the patient’s visit. By ensuring that patients provide thorough information, healthcare providers can better tailor their care and make informed decisions during the consultation.
The Patient Medical History form shares similarities with the Annual Physical Examination form, focusing on the patient's past and present health conditions. This form usually requires patients to detail previous surgeries, chronic illnesses, and family medical history. Like the Annual Physical Examination form, it aims to provide a complete picture of the patient’s health, enabling doctors to identify potential risks and tailor their approach to treatment. Both documents emphasize the importance of understanding a patient’s health background for effective medical care.
The Immunization Record is another document closely related to the Annual Physical Examination form. This record tracks vaccinations a patient has received, including dates and types of immunizations. Similar to the immunization section of the Annual Physical Examination form, it is crucial for ensuring that patients are up-to-date with their vaccinations. This information is vital for preventing disease outbreaks and for public health monitoring, underscoring the importance of maintaining accurate and current immunization records.
The Consent for Treatment form bears resemblance to the Annual Physical Examination form as both require patient signatures to confirm understanding and agreement. The Consent for Treatment form typically outlines the procedures and potential risks associated with medical treatments. Like the Annual Physical Examination form, it emphasizes the patient's active participation in their healthcare decisions. Both documents are essential for establishing a clear understanding between healthcare providers and patients, fostering trust and transparency in the medical process.
The Health Risk Assessment (HRA) is another document that aligns with the Annual Physical Examination form by evaluating a patient’s risk factors for various health conditions. The HRA typically includes questions about lifestyle habits, family history, and existing health issues. Similar to the Annual Physical Examination form, it aims to identify areas where patients may need to focus on improving their health. By assessing risk factors, healthcare providers can recommend preventive measures and tailor health interventions to better meet the individual needs of patients.
When filling out the Annual Physical Examination form, it is important to ensure accuracy and completeness. Here are some helpful tips on what to do and what to avoid:
Here are seven common misconceptions about the Annual Physical Examination form. Understanding these can help you navigate the process more smoothly.
Many believe that filling out the Annual Physical Examination form is not necessary. In reality, providing complete information is crucial to ensure a thorough evaluation during your appointment.
Some think that only first-time patients need to complete the form. However, returning patients should also update their information to reflect any changes in health or medications.
While personal details are important, the form also asks for medical history, current medications, and any allergies. This information helps the physician provide better care.
Some people feel pressured to complete every section each year. If there are no changes in certain areas, you can indicate that by marking the appropriate boxes.
It's a common belief that only major health problems should be included. However, even minor issues or concerns can impact overall health and should be mentioned.
Many assume that this form is only for adults, but children and adolescents also require physical examinations. Their forms will have similar requirements.
While some may think they can complete the form at the doctor's office, it's best to fill it out beforehand. This ensures that you have enough time to provide accurate and thoughtful responses.
Filling out the Annual Physical Examination form is an important step in maintaining your health. Here are some key takeaways to keep in mind:
By following these guidelines, you can help ensure a smoother experience during your annual physical examination.