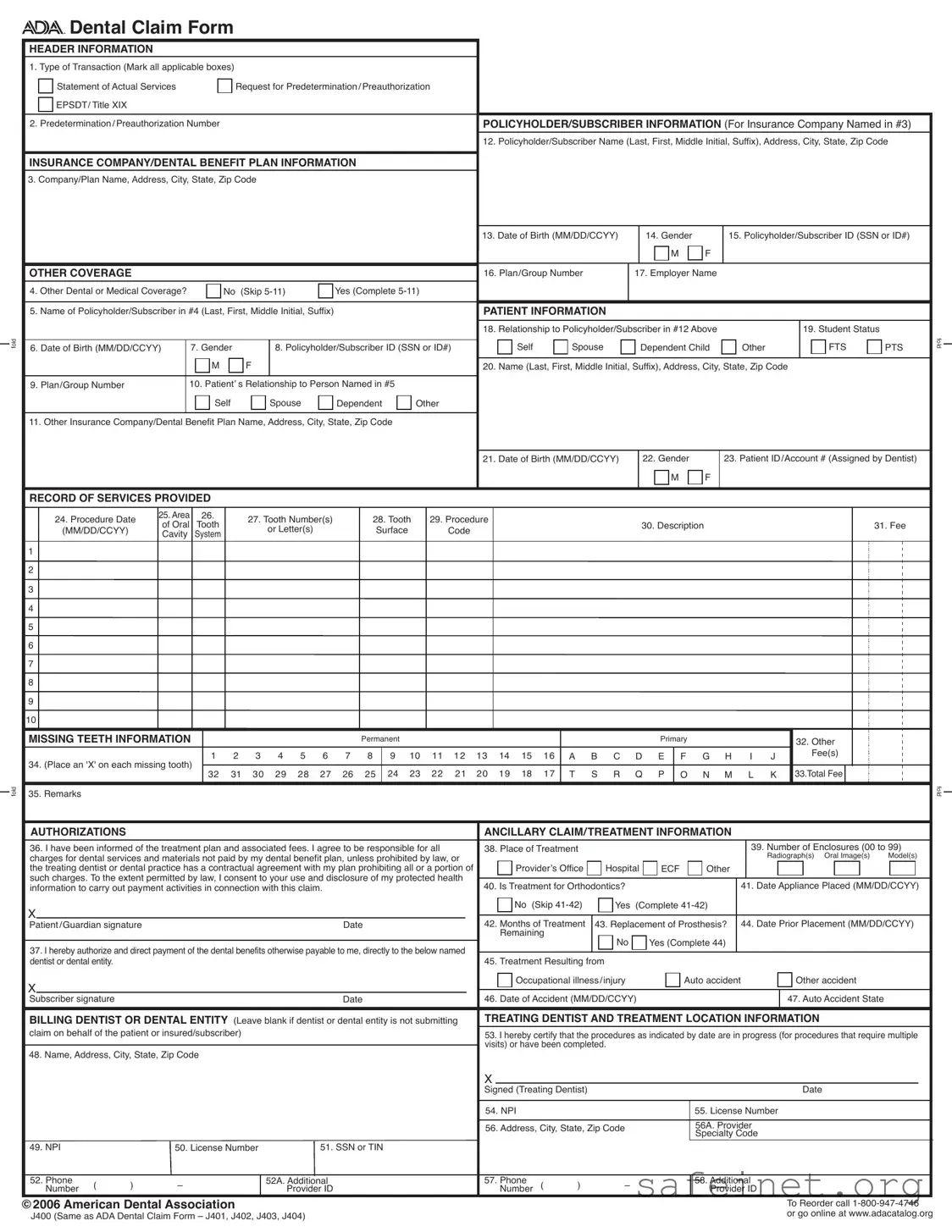
The ADA Dental Claim Form serves as a vital document in the process of submitting dental claims to insurance companies and dental benefit plans. It encompasses several key sections that gather essential information about the transaction type, policyholder, patient, and the services rendered. The form begins with header information, where individuals indicate the type of transaction, such as a statement of actual services or a request for predetermination. Following this, the policyholder's details are captured, including their name, address, and insurance information. Additional sections address other coverage that may exist, alongside patient-specific information like their relationship to the policyholder and their demographic details. The record of services provided is a crucial part of the form, detailing the procedures performed, associated fees, and any missing teeth information. The ADA Dental Claim Form also includes authorizations and ancillary treatment information, ensuring that all necessary consents are obtained for the processing of claims. Proper completion of this form is essential, as it streamlines the claims process and facilitates timely reimbursement for dental services rendered.
| Fact Name | Details |
|---|---|
| Form Purpose | The ADA Dental Claim Form is used to submit claims for dental services to insurance companies or dental benefit plans. |
| Transaction Types | Users can indicate multiple transaction types, including Statement of Actual Services and Request for Predetermination/Preauthorization. |
| Policyholder Information | Details such as the policyholder's name, address, and subscriber ID must be provided for insurance processing. |
| Patient Information | Information about the patient, including their relationship to the policyholder and date of birth, is required. |
| Record of Services | The form includes sections to detail the services provided, including procedure dates and associated fees. |
| Missing Teeth Information | Claimants must indicate any missing teeth on the form by marking the appropriate boxes. |
| Coordination of Benefits | If applicable, the form must be completed in full when submitting to a secondary payer, along with the primary payer's Explanation of Benefits. |
| National Provider Identifier (NPI) | Dentists must include their NPI, which is a unique identifier assigned by the federal government. |
| Provider Specialty Codes | Specialty codes indicate the type of dental professional who provided treatment, such as orthodontics or pediatric dentistry. |
| State-Specific Requirements | Some states may have additional laws or regulations that govern the use of the ADA Dental Claim Form. It is essential to check local laws. |
Filling out the ADA Dental Claim form is an important step in ensuring your dental services are covered by your insurance. Follow these steps carefully to complete the form accurately.
What is the purpose of the ADA Dental Claim Form?
The ADA Dental Claim Form is primarily used to submit claims for dental services provided to patients. It allows dental professionals to request payment from insurance companies or dental benefit plans. The form collects essential information about the patient, the policyholder, and the services rendered. By using this standardized form, dental practices can ensure that claims are processed efficiently and accurately, reducing the likelihood of delays in payment.
What information is required on the ADA Dental Claim Form?
Completing the ADA Dental Claim Form requires several pieces of information. Key sections include header information about the type of transaction, policyholder and subscriber details, and patient information. Additionally, the form asks for specifics regarding the services provided, such as procedure dates, tooth numbers, and associated fees. It is important to fill out all applicable sections to prevent any issues with claim processing.
How should the ADA Dental Claim Form be submitted?
The form should be folded according to the tick-marks provided in the margin to ensure that the insurance company’s name and address are visible in a standard #10 envelope. After completing the form, it can be mailed directly to the dental benefit plan or insurance company. If the claim is being submitted to a secondary payer, it is necessary to include the primary payer’s Explanation of Benefits (EOB) along with the completed form.
What should I do if there are multiple procedures to report?
If the number of procedures exceeds the lines available on a single ADA Dental Claim Form, it is important to complete an additional form for the remaining procedures. Each form must be fully completed to ensure that all services are documented and can be reviewed by the insurance company. This helps in maintaining clarity and accuracy in the claims process.
What is the National Provider Identifier (NPI) and why is it important?
The National Provider Identifier (NPI) is a unique identifier assigned to healthcare providers, including dentists, by the federal government. It is essential for billing and claims processing, as it helps to identify providers in a standardized manner. Dentists are required to include their NPI on the ADA Dental Claim Form if they are considered HIPAA covered entities. This helps streamline communication between dental practices and insurance companies, facilitating quicker and more efficient processing of claims.
Incomplete Header Information: Failing to mark all applicable transaction types can lead to processing delays. Ensure that you select all that apply, including Statement of Actual Services and Request for Predetermination.
Missing Policyholder Information: Omitting the full name and address of the policyholder can cause issues. Always provide the last name, first name, middle initial, and suffix, along with the complete address.
Incorrect Date Formats: Dates must be entered in the MM/DD/CCYY format. Using an incorrect format can result in rejections or delays.
Not Indicating Other Coverage: If there is other dental or medical coverage, it's crucial to indicate this and complete the relevant sections. Failing to do so may affect claim processing.
Missing Patient Information: Ensure that all patient details, such as name, relationship to the policyholder, and date of birth, are fully completed. Incomplete patient information can lead to claim denials.
Neglecting to List Multiple Procedures: If the number of procedures exceeds the lines available on the form, additional procedures must be documented on a separate claim form. Skipping this step can complicate the claim process.
Ignoring the Remarks Section: Use the remarks field to provide any necessary explanations or additional information, especially when submitting to a secondary payer. This can facilitate smoother processing.
Forgetting Signatures: Claims must be signed by both the patient or guardian and the treating dentist. Missing signatures can halt the claim process.
Not Using the Correct Provider Identifier: Make sure to include the correct National Provider Identifier (NPI) and any additional provider identifiers. Incorrect identifiers can lead to claim rejections.
The ADA Dental Claim Form is an essential document for submitting dental insurance claims. However, it is often accompanied by other forms and documents that help streamline the claims process. Below are five commonly used documents that may be needed alongside the ADA Dental Claim Form.
These documents play a vital role in ensuring that dental claims are processed smoothly and efficiently. Having them ready can help avoid delays and misunderstandings, making the experience easier for both patients and dental providers.
The ADA Dental Claim Form shares similarities with the CMS-1500 form, which is used for medical claims in the United States. Both forms require detailed patient and provider information, including names, addresses, and identification numbers. They serve as essential tools for healthcare providers to submit claims to insurance companies for reimbursement. Each form also includes sections for documenting the services provided, ensuring that the payer has a clear understanding of the treatment rendered and the associated costs. The structured layout of both forms aids in efficient processing by insurers, facilitating quicker payment for services rendered.
Another document comparable to the ADA Dental Claim Form is the UB-04 form, primarily used for institutional healthcare claims. Like the ADA form, the UB-04 captures vital information about the patient, provider, and services rendered. Both documents require comprehensive details about the treatment and associated costs. However, while the ADA form is tailored for dental services, the UB-04 addresses a broader range of healthcare services, including inpatient and outpatient hospital care. This distinction highlights the specific focus of each form while maintaining a similar purpose in facilitating claims processing.
The Dental Treatment Plan is another document that aligns closely with the ADA Dental Claim Form. This plan outlines the recommended dental services for a patient, detailing procedures, costs, and timelines. While the ADA form is used to claim reimbursement for completed services, the treatment plan serves as a proactive measure to inform both the patient and the insurer of expected procedures and associated fees. Both documents emphasize clear communication and transparency between dental providers and insurance companies, ensuring that all parties are aware of the treatment process and financial responsibilities.
The Health Insurance Claim Form (HICF) is also similar to the ADA Dental Claim Form, as it is utilized across various healthcare settings to submit claims for reimbursement. Both forms require essential information about the patient, provider, and services provided. The HICF encompasses a wider range of medical services, while the ADA form is specifically designed for dental care. Despite this difference, both forms streamline the claims process, ensuring that insurers have the necessary details to evaluate and process claims efficiently.
Lastly, the Explanation of Benefits (EOB) document complements the ADA Dental Claim Form. While the ADA form is used to submit claims, the EOB provides a breakdown of the insurance company’s response to those claims. It outlines the services covered, the amount paid, and any remaining patient responsibilities. Both documents work together to ensure clarity in the claims process, allowing patients and providers to understand the financial aspects of dental care. The EOB serves as a crucial communication tool that follows the submission of the ADA form, ensuring all parties are informed of the outcomes related to the claim.
When filling out the ADA Dental Claim Form, attention to detail is crucial. Here are ten important things to keep in mind:
By following these guidelines, the chances of a smooth claims process increase significantly. Careful attention to detail will help ensure that the claim is processed efficiently and accurately.
Misconceptions about the ADA Dental Claim Form can lead to confusion and errors in submissions. Here are four common misunderstandings:
Ensure you fill out all required fields on the ADA Dental Claim Form. Missing information can delay processing.
Clearly indicate the type of transaction by marking the appropriate boxes. This helps the insurance company understand the purpose of the claim.
Provide complete and accurate patient and policyholder information, including names, addresses, and identification numbers. This is crucial for proper identification.
If there is other dental or medical coverage, make sure to complete the relevant sections. This ensures coordination of benefits and proper payment.
Use the Remarks section to include any additional information, such as the amount paid by a primary insurer if submitting to a secondary payer.
Familiarize yourself with the National Provider Identifier (NPI) requirements. This identifier is essential for claims submitted by dental professionals.