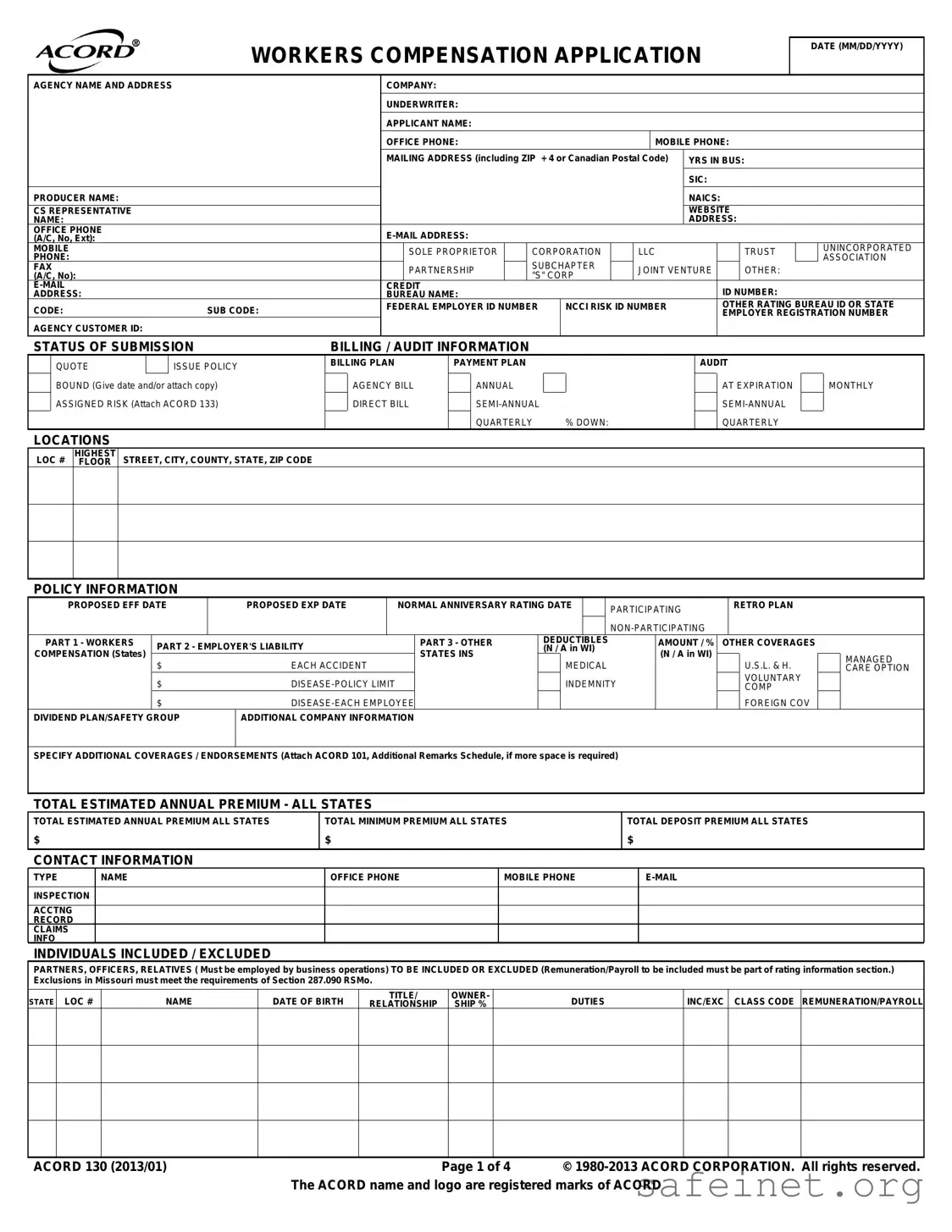
The Acord 130 form serves as a vital tool in the workers' compensation insurance application process, capturing essential information about a business seeking coverage. This form requires details such as the applicant's name, agency information, and contact details. It also collects data on the type of business entity, years in operation, and relevant classification codes. Furthermore, the Acord 130 includes sections for providing information on estimated annual premiums, prior insurance history, and any loss history over the past five years. The form prompts applicants to disclose specific operational details, including the nature of their business, employee classifications, and any unique risks associated with their operations. Additionally, it addresses billing preferences and coverage options, ensuring that applicants are aware of their choices regarding payment plans and policy terms. By thoroughly completing the Acord 130, businesses can facilitate a smoother application process, ultimately leading to the appropriate workers' compensation coverage tailored to their needs.
| Fact Name | Details |
|---|---|
| Purpose | The ACORD 130 form is used for applying for workers' compensation insurance, providing necessary information about the applicant's business and coverage needs. |
| Required Information | The form requires detailed information including the applicant's name, business type, contact information, and estimated annual payroll. |
| State-Specific Regulations | Each state may have specific requirements governing the use of the ACORD 130 form, including compliance with local workers' compensation laws. |
| Exclusions and Inclusions | The form allows applicants to specify individuals to be included or excluded from coverage, which is crucial for accurate premium calculations. |
| Fraud Warning | The form includes a warning about the consequences of providing false information, which can lead to legal penalties and denial of coverage. |
Completing the Acord 130 form is an essential step in applying for workers' compensation insurance. This form collects vital information about your business, including contact details, coverage needs, and employee information. Filling it out accurately ensures that your application is processed smoothly and helps avoid any delays in obtaining your insurance.
What is the Acord 130 form used for?
The Acord 130 form is primarily used to apply for workers' compensation insurance. It collects essential information about a business, including its operations, employee details, and coverage needs. Insurers use this information to assess risk and determine appropriate premium rates for the coverage requested.
What information is required on the Acord 130 form?
The form requires various details, such as the applicant's name, business structure, contact information, and years in business. Additionally, it asks for specifics about employee classifications, estimated payroll, and any previous insurance coverage or loss history. Accurate and complete information is crucial for a successful application.
Who should complete the Acord 130 form?
The form should be completed by an authorized representative of the business applying for coverage. This person is typically an owner, officer, or partner who can provide accurate information about the company's operations and employee details. Their signature is necessary to validate the application.
How does the Acord 130 form affect insurance premiums?
The information provided on the Acord 130 form directly impacts the calculation of insurance premiums. Insurers evaluate factors such as the nature of the business, employee classifications, and past claims history to determine the risk level. Higher risks may lead to increased premiums, while lower risks could result in more favorable rates.
What happens after submitting the Acord 130 form?
Once the Acord 130 form is submitted, the insurance company will review the application. They may request additional information or clarification on certain points. After assessing the risk, the insurer will provide a quote for the workers' compensation coverage, outlining the terms, conditions, and premium amount.
Can the Acord 130 form be modified after submission?
Yes, if there are significant changes in the business operations or employee details after submitting the Acord 130 form, the applicant should notify the insurance company. Adjustments may be necessary to ensure that the coverage remains adequate and reflects the current risk profile of the business.
Incorrect Date Format: Ensure the application date is entered in MM/DD/YYYY format. Using an incorrect format can lead to processing delays.
Missing Contact Information: Always provide complete contact details. This includes office phone, mobile phone, and email address. Incomplete information can hinder communication.
Omitting Business Structure: Clearly indicate the type of business entity (e.g., corporation, LLC, partnership). Failing to specify can lead to misclassification.
Neglecting to List All Employees: Include all employees in the payroll section. Excluding employees can result in inaccurate premium calculations.
Incorrect SIC/NAICS Codes: Use accurate SIC and NAICS codes that reflect your business activities. Incorrect codes can affect your insurance rates.
Not Specifying Coverage Needs: Clearly outline any additional coverages or endorsements required. Missing this information may lead to insufficient coverage.
Failure to Attach Required Documents: Always attach necessary documents, such as loss runs or additional remarks. Omitting these can delay processing.
Ignoring Prior Carrier Information: Provide complete information about previous insurance carriers and loss history. This helps in evaluating your risk profile.
Inaccurate Payroll Estimates: Provide realistic payroll estimates for all employees. Underestimating payroll can lead to unexpected premium adjustments.
Not Signing the Application: Ensure the application is signed by an authorized representative. An unsigned application is not valid and will be rejected.
The ACORD 130 form is essential for workers' compensation insurance applications. Several other forms and documents are often used in conjunction with it to ensure a comprehensive submission. Below is a list of these related documents, along with brief descriptions of each.
These documents work together with the ACORD 130 form to facilitate a thorough application process for workers' compensation insurance. Ensuring all necessary information is provided can help streamline the underwriting process and secure appropriate coverage.
The ACORD 125 form serves as a standard application for commercial insurance. Like the ACORD 130, it collects essential information about the applicant's business, including contact details, type of business entity, and coverage needs. Both forms are designed to streamline the underwriting process by ensuring that insurers have the necessary information to assess risk and provide accurate quotes. The ACORD 125 focuses on a broader range of coverages, while the ACORD 130 specifically targets workers' compensation and employer's liability insurance.
The ACORD 133 form is specifically used for assigned risk applications in workers' compensation insurance. Similar to the ACORD 130, it requires detailed information about the applicant's business operations, employee classifications, and payroll estimates. Both forms are essential in determining eligibility for coverage and calculating premiums. The ACORD 133 complements the ACORD 130 by providing additional context for businesses that may not qualify for standard coverage options.
The ACORD 101 form, known as the Additional Remarks Schedule, allows applicants to provide further details or clarifications regarding their insurance needs. This form is similar to the ACORD 130 in that it helps capture additional information that may be necessary for the underwriting process. While the ACORD 130 focuses on specific insurance coverages, the ACORD 101 provides a space for applicants to elaborate on unique circumstances or special requests that could affect their coverage.
The ACORD 140 form is utilized for commercial property insurance applications. While the ACORD 130 centers on workers' compensation, both forms require similar foundational information about the applicant's business, including location, type of business, and coverage limits. The ACORD 140, however, emphasizes property-related risks, while the ACORD 130 focuses on employee-related risks, reflecting the different aspects of insurance coverage they address.
The ACORD 150 form is designed for general liability insurance applications. Like the ACORD 130, it gathers vital information to help insurers assess risk and determine appropriate coverage. Both forms require details about the business's operations, including the nature of the work performed and any associated risks. The ACORD 150, however, is specifically tailored to liability coverage, whereas the ACORD 130 is dedicated to workers' compensation and employer's liability.
The ACORD 200 form serves as a personal auto application. While it is targeted toward individual insurance needs rather than business operations, it shares similarities with the ACORD 130 in terms of gathering necessary personal information, coverage options, and vehicle details. Both forms aim to facilitate the underwriting process by ensuring that all relevant data is collected upfront, allowing for a smoother and more efficient application experience.
When filling out the ACORD 130 form, there are several key points to keep in mind. Here’s a list of things you should and shouldn’t do:
Misconception 1: The Acord 130 form is only for large businesses.
This form is designed for all types of businesses, regardless of size. Small businesses can and should use the Acord 130 to ensure they have the appropriate workers' compensation coverage. It helps to accurately assess risks and premiums, making it relevant for any business owner.
Misconception 2: Completing the Acord 130 form is optional.
For businesses that require workers' compensation insurance, submitting the Acord 130 is often a necessary step in the application process. It provides essential information that insurers need to evaluate risk and determine coverage. Skipping this form can lead to delays or complications in obtaining coverage.
Misconception 3: The Acord 130 form only focuses on employee information.
While the form does require details about employees, it also encompasses various aspects of the business, including operations, prior claims history, and specific business activities. This comprehensive approach allows insurers to gain a full understanding of the business's risk profile.
Misconception 4: Errors on the Acord 130 form can be easily corrected after submission.
While it is possible to amend information, inaccuracies can lead to significant issues, including policy delays or incorrect coverage. It is crucial to review the form carefully before submission to ensure that all information is accurate and complete.
Accurate completion of the Acord 130 form is crucial for obtaining the right workers' compensation coverage. Ensure all fields are filled out completely and correctly.
Include contact information for all relevant parties, such as the applicant, agency, and underwriter. This facilitates communication and speeds up the processing of your application.
Provide a detailed loss history for the past five years. This information is vital for underwriters to assess risk and determine premiums.
Be transparent about any exclusions or special circumstances, such as subcontracting work or unique operational risks. This can prevent complications later in the process.
Review the general information section carefully. Answer all questions honestly, as inaccuracies can lead to coverage denial or penalties.